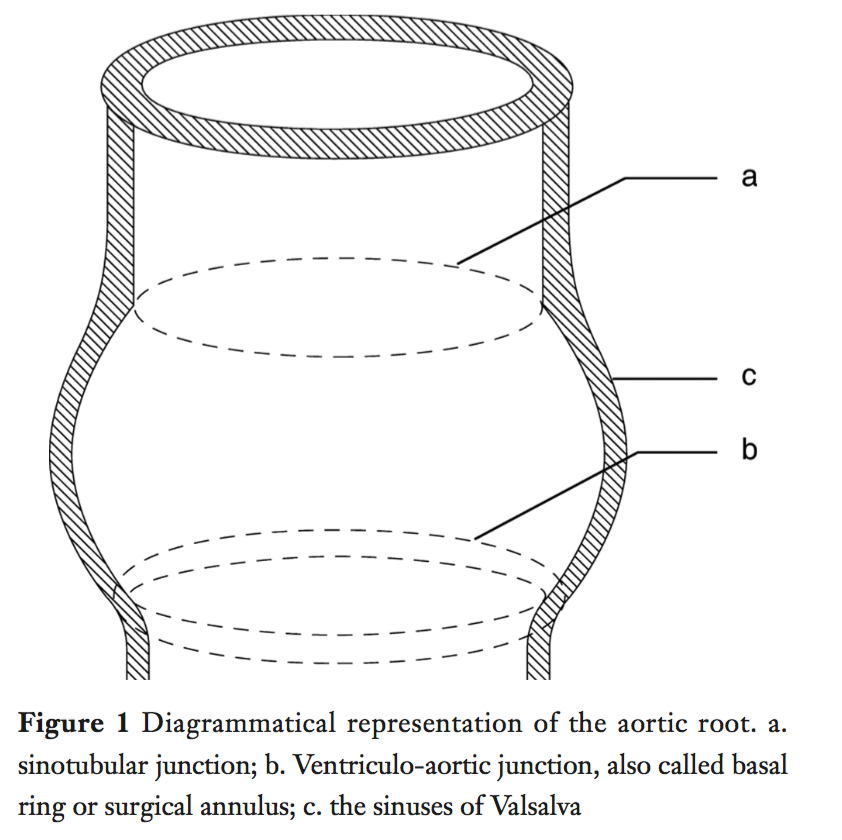
Aortic root (aka functions aortic annulus) – lower limit is the ventricle-aortic junction (VAJ, aka surgical annulus) & upper limit is the sinotubular junction (STJ)
Normal VAJ area changes during cardiac cycle – increased during isovolumetric contraction & ejection, decreased during isovolumetric relaxation, increased during diastole
Normal aortic annulus is oval & becomes more circular with dilation
The annulus is larger in a bicuspid AV than a tricuspid AV
The annulus becomes progressively larger with increased degree of AR
Originally used glutaraldehyde-treated autologous pericardium for reconstruction
Cardiocel (bovine pericardium) has been used successfully in congenital heart surgery for 8 years
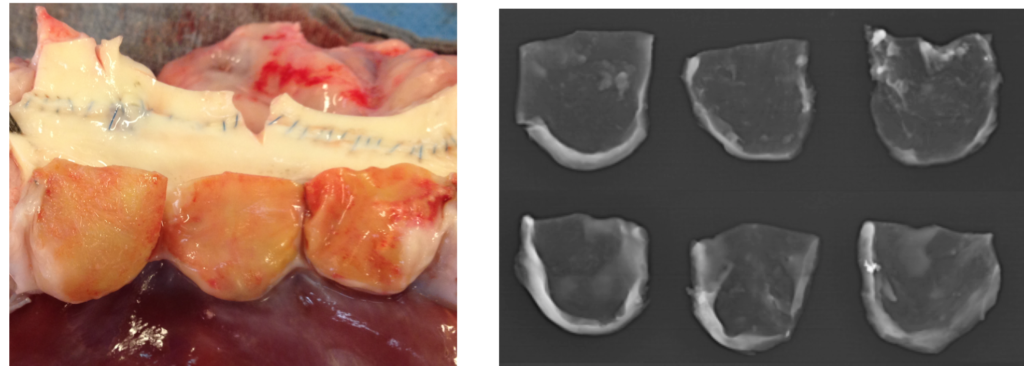
Study looked at performing the Ozaki operation using Cardiocel in sheep
Echo at 6 months showed valves functioning well
Explant showed preserved structure & stability of the Cardiocel tissue
Low rate of calcification
Neo-intima formation & re-cellularisation with host cells
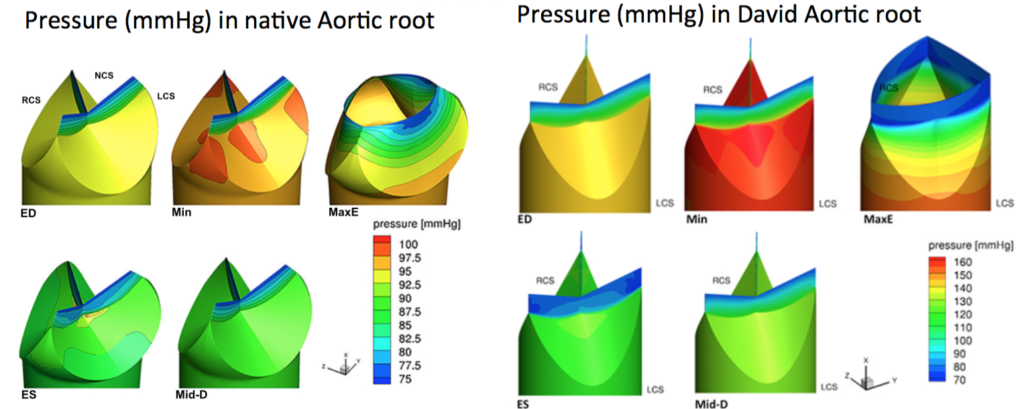
Haemodynamics of David procedure
3D aortic root geometry & flow dynamics were assessed during the cardiac cycle in pigs with native aortic root or David procedure
The David root is exposed to high pressures & low shear stress for a longer time during the cardiac cycle than the native aortic root, which would favour degeneration
However clinical outcomes have of the David have been very good – perhaps there is leaflet remodelling that occurs in response to this pressure
Not presented specifically, but apparently when same model was applied to the Yacoub repair the haemodynamic profile was superior to the David & closer the native aortic root
Atrio-Ventricular Valves
Parachute ventricular partitioning
Used to partition off & exclude an apical aneurysm & increase EF
Nitinol-based PTFE covered parachute-like device
Transfemoral delivery
Guide catheter points at the landing zone in the ventricular apex, the device is deployed, & a balloon is used to expand the nitinol frame
Transcatheter Mitral Valve Implantation (TMVI)
Number of differences in the MV compared to the AV that makes designing transcatheter devices challenging
Differences in anatomy
Larger size & D shape
Complex subvavular apparatus
Some cords insert into the leaflet body rather than the free margin, the anterior commissure is close to the AV,
The MV is also close to the circumflex artery
Differences in physiology
MV separates low-resistance from high-resistance, whilst AV separates high-resistance from high-resistance
MV has low-resistance inflow (diastole) & high-resistance outflow (systole)
Annulus changes dimensions up to 40% in systole
Both aetiology & affected structures are highly varied
Differences in design priorities
Aim to decrease or maintain the EOA, as opposed to maximising
The height of the device affects risk of LVOTO
The angle of the device to the AV also affects risk of LVOTO
Size of ventricle affects how much room there is for the device
TMVI – CardiAQ (Edwards Lifesciences)
Bovine pericardial trileaflet valve with intra-annular sealing skirt to minimise PVL
Ventricular part delivered first, then whole valve is pushed up into the annulus, then atrial part delivered
Transapical or transatrial delivery
Self centuring & self positioning on release
First in man planned for next month
Tricuspid valve repair
The TV tends to dilate in the anterior & posterior leaflet direction (I.e not in the septal leaflet direction)
Bicuspidation of the tricuspid valve technique
Mattress sutures from the mid point of the posterior leaflet to the mid point of the septal leaflet
No difference in survival compared to annuloplasty
Mitralign transcather device for tricuspid annuloplasty
Insertion made using RF
First insertion make around the posterior-septal commisure
Device is sinched down 2 plegetted sutures & creates annuloplasty
Max distance to sinch (I.e between sutures) is 2.8cm – the tricuspid annular tissue is more fragile than mitral annular tissue, & any more distance could be damaging
Makes the posterior leaflet redundant
Used in 10 patients worldwide
Tricuspid valve repair using extra cellular matrix cylinder
Heart Failure Surgery
Heartmate III CE mark trial
Uses Maglev technology to magnetically suspend the impeller (no hydrodynamic or mechanical bearings) – allows for wide range of flow, artificial pulse (hopefully less aortic insufficiency, blood stasis, fewer GI bleeds), more consistent pump gaps (hoping to reduce haemolysis & thrombosis)
First in-human trial, prospective, non-randomised, n=60
Mean age 59yrs, ischaemic aetiology in 44%
All implants via median sternotomy
Drive line externalised with silicone to skin interface in 96% (designed to reduce infection)
42% had concomitant procedures (valve operations, PFO, LAA occlusion)
mean CPB time 84min (63-110)
30 day outcomes
Bleeding 30%
Quite high due to strict definition (≥4 units in first 7 days, ≥1 unit after day 7)
12% required reoperation
Stroke 4% – 1 patient had difficulty engaging inflow conduit; 1 ischaemic stroke from anaphylactic shock
8% right heart failure (2 requiring RVAD support)
No device malfunction, thrombosis, haemolysis
98% survival (1 death in the ischaemic stroke patient)
6 month endpoint also met, awaiting CE mark approval
In Viena (where study was) as soon as CE mark they will stop implant Heartmate II & only use III
Lavare cycle in the HeartWare HVAD
Lavare cycle involves periodic speed modulation which may reduce blood stasis
Lower speed (-200rpm) for 2 sec, then higher speed (+200rpm) for 1 sec, then baseline for 60sec, then cycle starts again
Step 1 – large vortex results in ventricular washout
Step 2 –
Step 3 – large ventricular washout again then normalised flow
ReVOLVE registry (n=248) analysis of the Lavare cycle
Significantly fewer stroke, sepsis, RHF
Other outcomes including survival were similar
Usually turned on after the patient leaves the OR (in Vienna)
Novel inflow cannula implant technique
LVAD results in servely disrupted blood flow in the LV – bloods flows to the ventriclar apex instead of the AV valve, increasing the risk of thrombosis
Study used an ex vivo dilated porcine heart (non-beating) on ECMO 4.5L
A cone shaped prosthetic tube was attached to the mitral valve annulus to funnel blood directly into the LVAD & avoid the disturbed flow in the LV
Resulted in higher flow rate & more streamlined elliptical shaped flow
Acute live animal experiment – successful implanted & weaned off CPB (onto VAD only) (animal had to be terminated at 1 hr due to ethics)
Next step is chronic animal model
LVAD less invasive approaches
Upper hemi-sternotomy + left thoracotomy approach possible
Helps preserve sternum for later heart transplantation
Alternative to hemi-sternotomy is right thoracotomy or right parasternal incision
Disadvantage is the outflow graft has to cross the midline twice as it travels to aorta
Disadvantage is more difficult access
Advantage is sternum is even further preserved for heart transplantation
Debate for sternotomy approach – David Adams, Mount Siani Medical Center, NY
Achieving 100% repair rate with no residual regurgitation is the most important priority
Some studies of the mini-thoracotomy approach have compromised repair rate or an increased rate of residual MR (3 or 4+) post repair
Handling complexities such as annular calcification is much more difficult through a mini-thoracotomy
To achieve good outcomes with mini or robotic mitral surgery you need to be at a super-high volume centre, which most places are not
Meta-analyses have found increased rate of stroke, possibly due to retrograde perfusion from femoral CPB cannulation
Limited sternotomy is not as morbid as the traditional full sternotomy but provides the same full open access, & has smaller incision with good cosmesis
Debate for minimally invasive approach – Patrick Perier, Herz und Gefäß Klinik, Germany
Mini-thoracotomy with direct vision still requires rib spreading which is still morbid & not as ‘minimally invasive’ as possible – so it should be done as port-access surgery with video vision
The exact same repair techniques should be replicated with the mini-thoracotomy approach
New programs need to be highly selective of simple patients at the beginning, then progressively add more complex repairs & concomitant procedures (e.g. AF) as they gain experience
Evidence on mini-mitrals – J Grau, Cleveland Clinic, USA
Intuity valve via upper hemi-sternotomy (n=51) vs. standard AVR via full sternotomy (n=49)
3 conversions to full sternotomy with scented bioprostheses – 2 unable to fit valve properly, 1 annulus tear
24% relative reduction in XC time (despite mini-incision, which usually increases XC time by 16%)
mortality not significantly different
PPM rate not significantly different, despite stent extending lower into the ventricle. Percival valve (similar sutureless valve) has higher PPM rate, but study had higher mean age than CADENCE-MIS (78 vs. 73), which may account for difference?
increased rate of mild PVL – potentially due to improper sizing, not aggressively debriding annular calcification
Intuity had significantly better EOA & gradients
Management of small aortic annulus
retrospective study comparing stented valves, Manougian procedure, stentless Freestyle prosthesis, & sutureless Percival S valve in patients with annulus <21mm
stentless group had significantly lower mean aortic gradient & higher EOA than other groups
this was a full root replacement with Freestyle graft, allowing for a larger prosthesis than the annulus
the Trifecta valve (St Jude) had significantly lower gradients & higher EOA than perimount, magna ease & mitroflow prostheses
Timing of individual steps in SAVR
aim to identify specific steps where time could be saved
exposure (stating after XC + AV assessment) – 5.3mm (10min)
resection (resection of AV leaflets + annulus decalcification + sizing) – 8.1mm (16%)
suturing – 17.3mm (33%)
tying – 9.1min (18%)
declamping – 11.9min (23%)
sutureless valves & knot tying devices have potential to significantly reduce time
Dr Michael Seco is a Cardiothoracic Surgery Registrar at Royal North Shore Hospital, Sydney, Australia. He has research interests in minimally-invasive cardiac surgical techniques, including robotic-assisted coronary artery bypass grafting, transcatheter aortic valve implantation, and off-pump surgery. Dr Seco also develops clinical databases.