Welcome to the monthly SHDA Research Update for March 2016. Our specialists have selected seminal papers that have been published recently in each specialty (cardiology, cardiothoracic surgery, cardiac imaging and perioperative medicine).
Cardiology
The first report of the one-year outcomes of the international REPRISE II (Repositionable Percutaneous Placement of Stenotic Aortic Valve through Implantation of Lotus Valve System–Evaluation of Safety and Performance) study is now available. This prospective, single-arm, multicentre trial enrolled patients >70 years with symptomatic severe aortic stenosis and NYHA functional class II or greater heart failure.
The Lotus Valve was used for transcatheter aortic valve replacement in this trial. This valve is marketed as ‘repositionable and retrievable’ and designed to ‘minimise paravalvular regurgitation.’ In 120 patients (mean age 84) at one year of follow-up 88.6% patients had no or trivial paravalvular aortic regurgitation and the all-cause mortality rate was 10.9%, disabling stroke rate was 3.4% and disabling bleeding rate was 5.9%.
It is important to note limitations including that the study design is not a randomised, double-blind, active-control trial and that the study was not statistically powered for clinical endpoints at one year.
This research study explores the use of real-time magnetic resonance imaging (rtMRI)-guided transcatheter aortic valve replacement (TAVR) in an animal model. The authors designed an MRI-compatible robot-assisted device to insert and deploy a self-expanding valve and tested it in 8 swine. A 12-mm trocar was inserted via a subxiphoid incision in the apex of the heart prior to entry to the MRI bore. Both the delivery device and nitinol stented prosthesis were mounted on the robot and real-time imaging provided virtual real-time 3-D reconstruction. Device deployment took on average 61 seconds. It was confirmed that there was full correlation between the valve position ascertained by imaging and the actual valve position at necropsy.
The authors concluded that: “This approach may eliminate some of the challenges of performing a procedure while working inside of an MRI scanner, and may improve the success of TAVR. It provides superior visualization during the insertion process, pinpoint accuracy of deployment, and, potentially, communication between the imaging device and the robotic module to prevent incorrect or misaligned deployment.”

Wazni O, Wilkoff BL. Considerations for cardiac device lead extraction. Nat Rev Cardiol. 2016 Apr
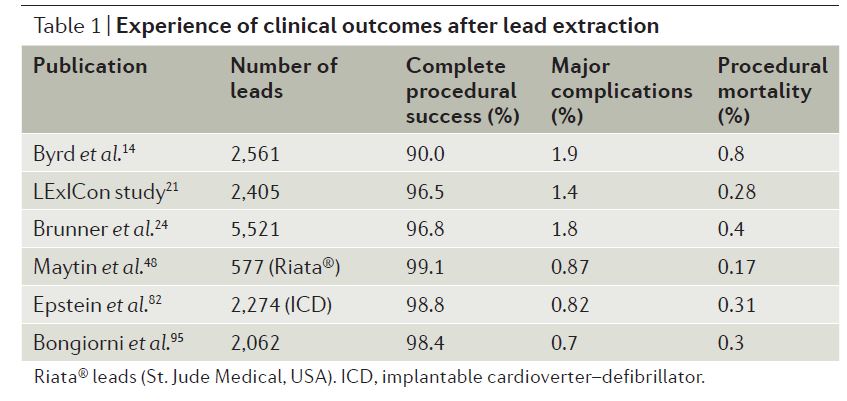
Extraction of cardiovascular implantable electronic device (CIED) leads is becoming a more common procedure with an estimated 20,000 performed worldwide each year. This article outlines indications for lead extraction and procedures commonly used for this purpose. Common reasons for extraction include infection, device recall, venous access and that the device has been superseded and the lead is no longer required. This article also presents a literature review of outcomes following lead extraction, including success and mortality rates.
Cardiothoracic Surgery
This systematic review and meta-analysis identified 12 eligible studies (8,661 patients) and examined the outcomes for patients undergoing aortic valve replacement with either a bioprosthetic valve (BV) or a mechanical valve (MV). Outcomes studied include long-term survival, major adverse prosthesis related events, anticoagulant-related events, major bleeding, reoperation, and structural valve degeneration. The authors concluded that: “Compared with MVs, BVs have reduced risk of major bleeding and anticoagulant-related events but increased risk of structural valve degeneration and reoperation.” They also noted that the findings of their review support the current trend toward using BVs in aortic valve replacement in patients >60 years.
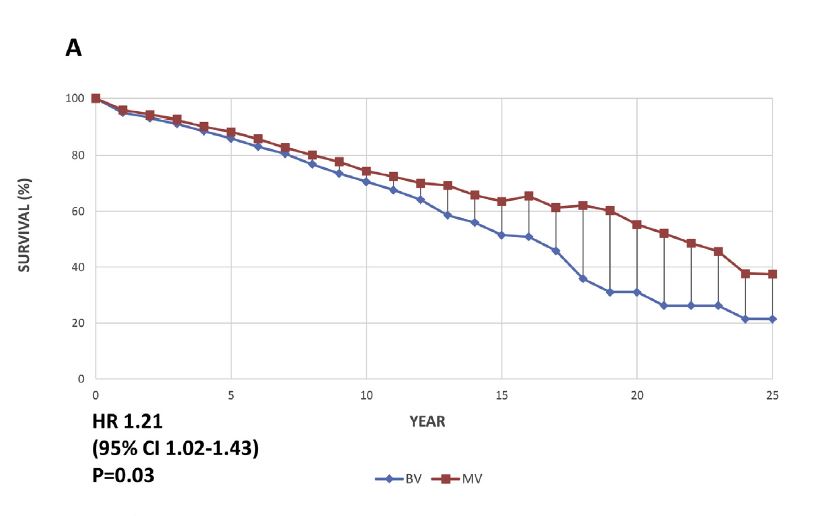
Figure A: Overall Kaplan-Meier survival curves based on reconstructed individual study data. (A) Aggregated survival curves for bioprosthetic valve (BV [blue line]) compared with mechanical valve (MV [red line]).
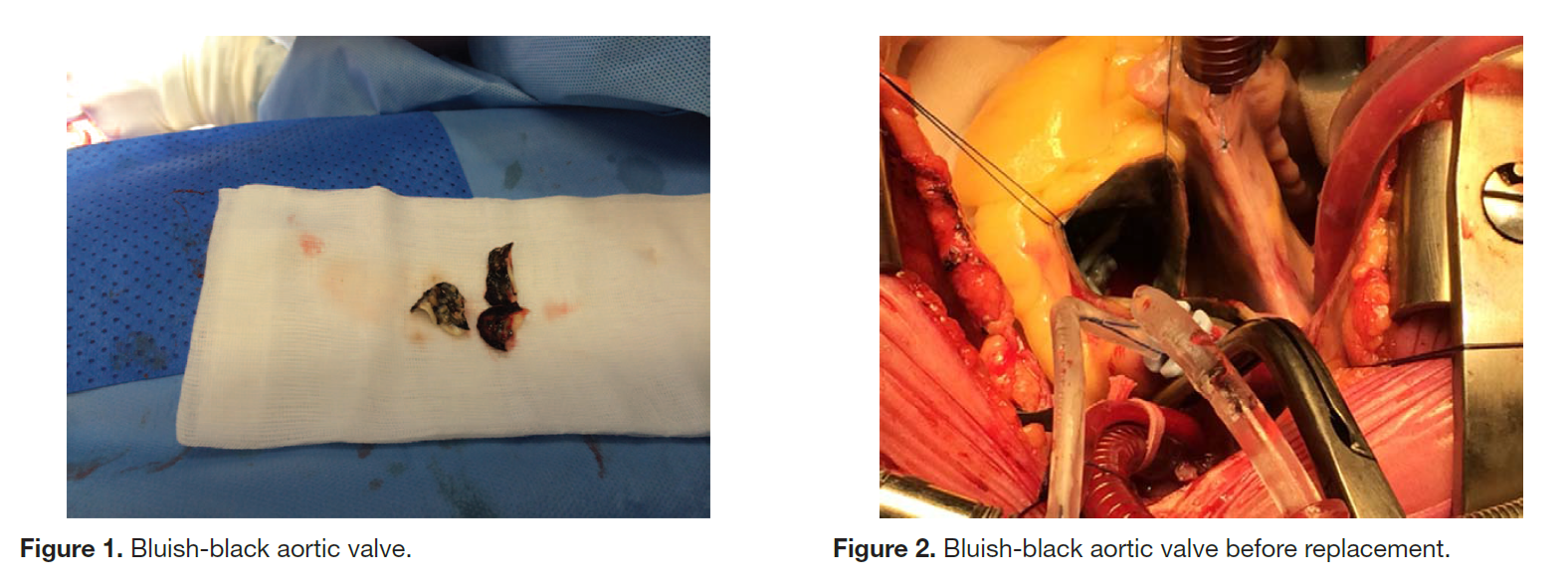
This report outlines a case of Alkaptonuria in a 72 year old woman who underwent aortic valve replacement for severe aortic valve stenosis. During surgery a black sternum was found and the aortic valve was a bluish-black colour. Alkaptonuric ochronosis is usually diagnosed at a younger age with black urine being the primary symptom. It is an inherited, recessive condition resulting from a deficiency in homogentisic acid oxidase. Alkaptonuric ochronosis is very rare except for populations in Slovakia and the Dominican Republic.
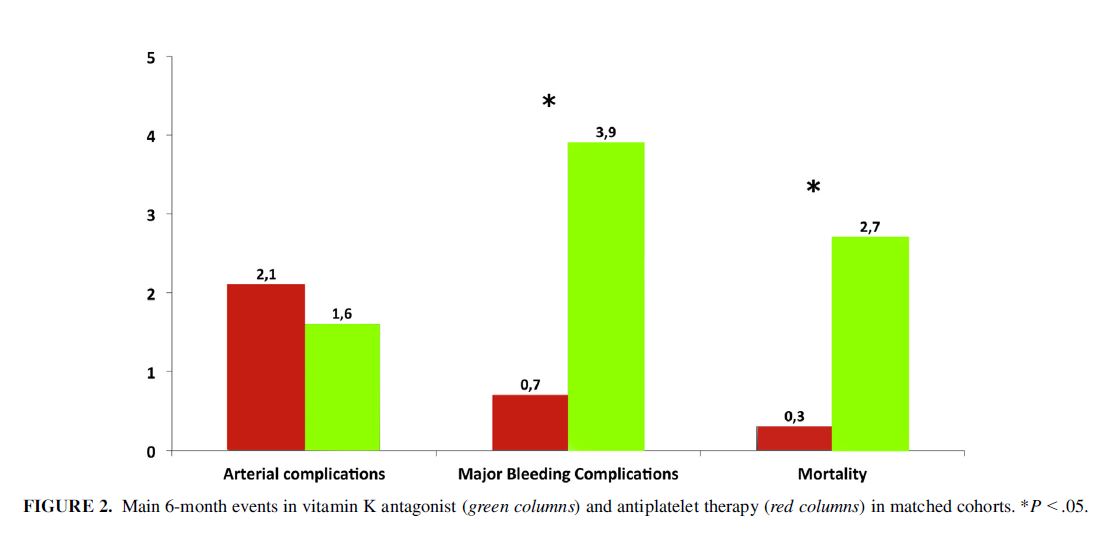
This multi-centre study collected data retrospectively from 19 institutions to investigate thromboembolic and haemorrhagic complications in the 6-month period following mitral valve repair. Different anti-thrombotic prophylaxis measures and patient outcomes were compared in 1,882 patients. In all, 1,517 were treated with an oral anticoagulant and 365 with antiplatelet drugs.
Patients receiving antiplatelet drugs were less likely to have major bleeding complications (3.9% vs 0.7%; P=0.01). It was also observed that the 6-month mortality rate was significantly higher in the oral anticoagulant (Vitamin-K agonist) group (2.7% vs 0.3%; P =0.02).
The authors concluded that: “Vitamin K antagonist therapy was not superior to antiplatelet therapy to prevent thromboembolic complications after mitral valve repair. Our data suggest that oral anticoagulation may carry a higher bleeding risk compared with antiplatelet therapy, although these results should be confirmed in an adequately powered randomized controlled trial.”
Cardiac Imaging
In this prospective study of 104 asymptomatic patients with moderate-severe aortic stenosis the prognostic value of global longitudinal strain (GLS) and basal longitudinal strain (BLS) was assessed. Multi-detector computed tomography (MDCT) coronary angiography was used to evaluate coexisting coronary pathology. Patients were followed-up for a median of 2.3 years and 43 patients (41%) met the criteria for aortic valve replacement indication for AVR. It was found that BLS, but not GLS, was a significant and independent predictor of future aortic valve replacement in asymptomatic patients with aortic stenosis.
This manuscript presents cardiac magnetic resonance derived normal reference values for the right ventricular (RV) volumes and systolic function. The study investigated the Framingham Heart Study Offspring cohort, which has been followed since 1971. Of 1,794 participants scanned using steady-state free precession cardiac magnetic resonance, a total of 1,336 adults were identified as free from cardiovascular and pulmonary disease. It was observed that RV volumes increase with body size, are greater in men, and are smaller in older people.