



Welcome to the monthly SHDA Research Update. Our specialists have selected 3 seminal papers that have been recently published in each speciality (Cardiology, Cardiac Surgery, Cardiac Imaging, Perioperative Medicine).
Cardiology
Summarised by Dr Sarah Catchpoole
This prospective study was conducted alongside the PARTNER 3 trial (patients with severe aortic stenosis, at low surgical risk, 1:1 randomisation to either SAVR or TAVR). 943 patient’s health status was assessed at baseline, 1, 6, and 12 months post intervention. Both groups had improved general health status and disease-specific health over one year. However, TAVR was associated with significant early improvements in disease-specific health compared to SAVR (16 point mean difference at 1 month, p<0.0001). This improvement was maintained, although less remarkable, at both 6 and 12 months (2.6 and 1.8 point mean difference, respectively, p<0.04 for both).
Takeaway: Compared to SAVR, TAVR is associated with better early disease-specific quality of life, with a modest advantage maintained at 6 and 12 months.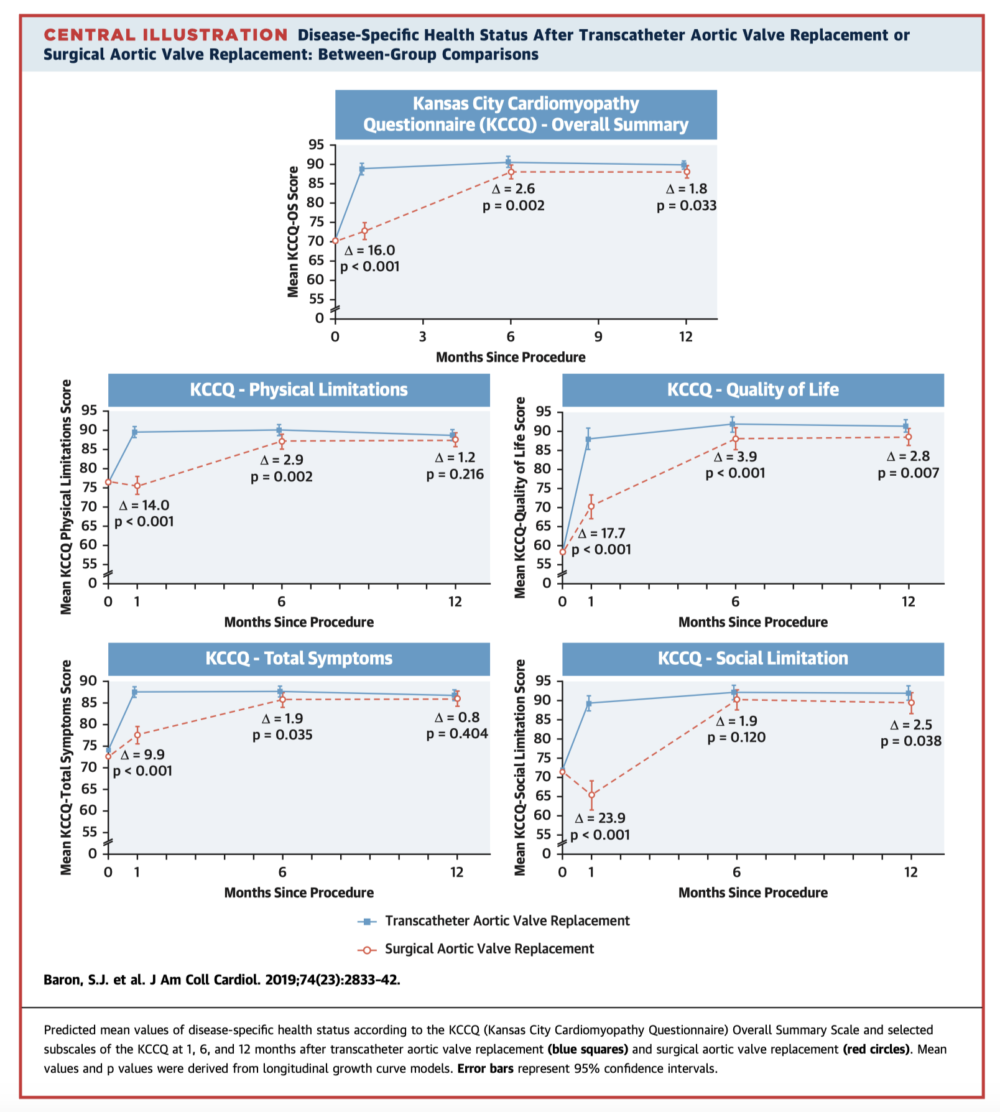
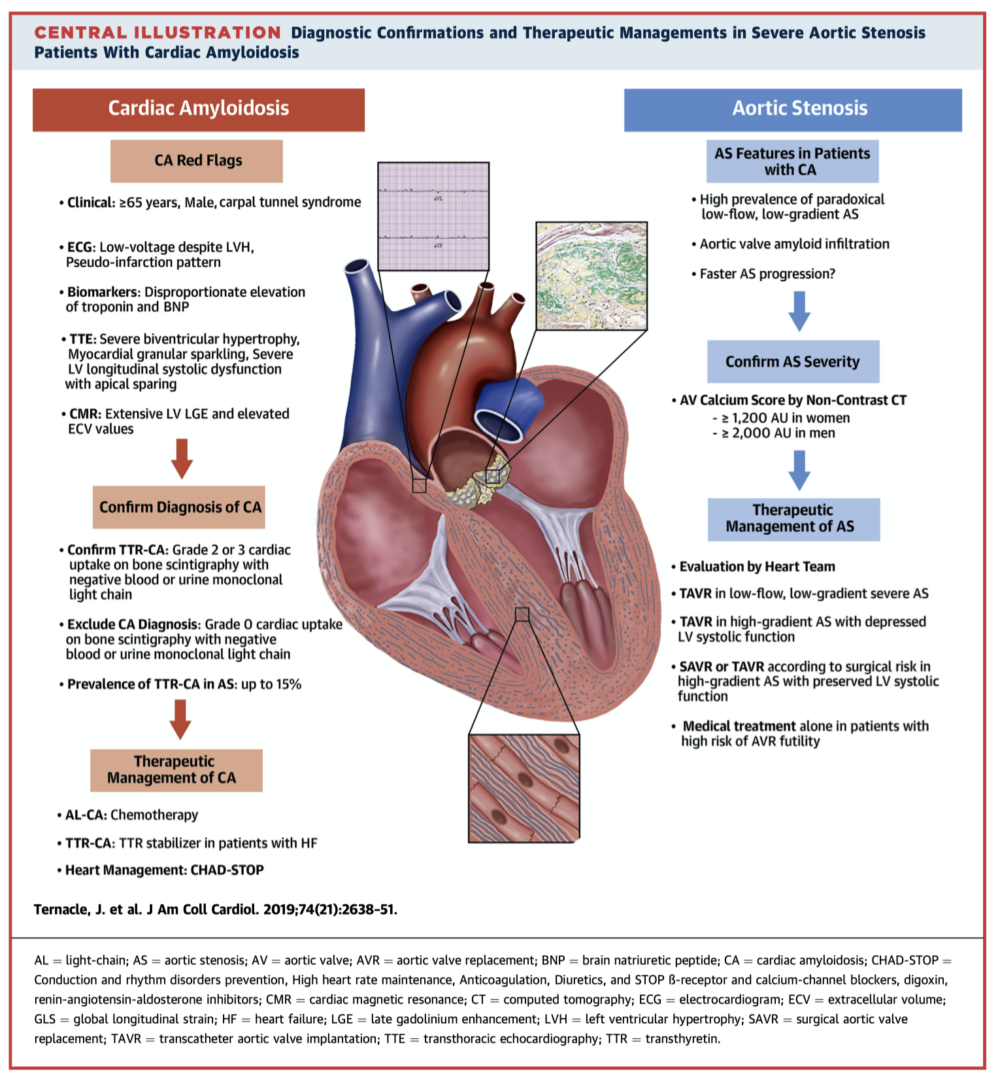
This review discusses the clinical overlap, diagnosis, and management of cardiac amyloidosis (CA) and aortic stenosis (AS). CA may be present in up to 15% of those with AS and has been associated with higher rates of heart failure, increased mortality, and treatment futility of surgical aortic valve replacement. Timely diagnosis of CA is also important given the emergence of new pharmacotherapies for transthyretin amyloidosis. The authors recommend systematic screening for “red flags” of CA in patients with AS; and these should trigger consideration of additional testing including serum free light chains and bone scintigraphy.
Takeaway: Cardiac amyloidosis and AS share several features, complicating diagnosis. Screen for “red flags” of CA in all patients with AS; these patients may benefit from the novel pharmacotherapies for transthyretin CA, and may be better suited to TAVR.
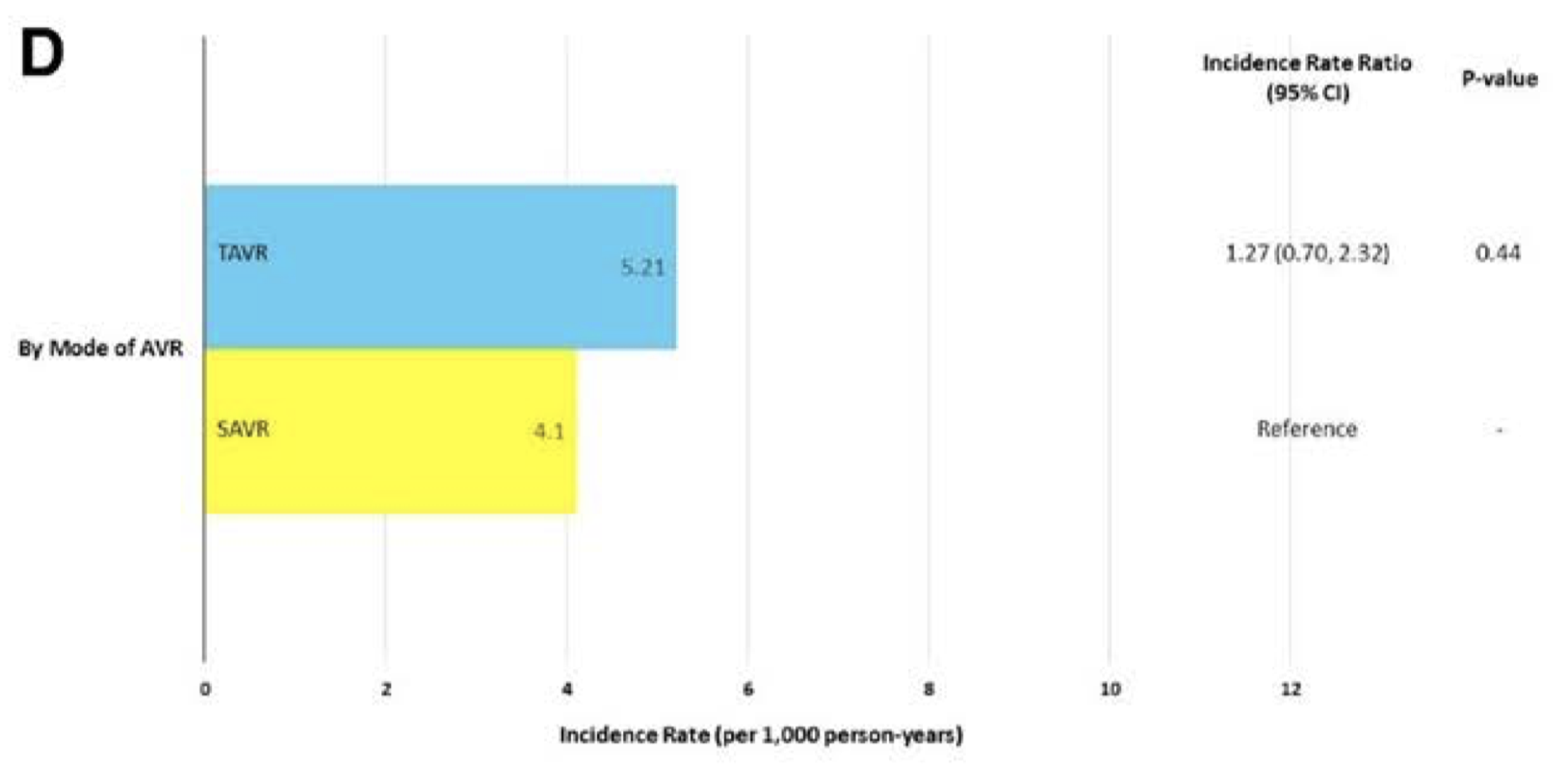
This paper analyses the incidence of prosthetic valve endocarditis (PVE) in patients with severe AS who received either SAVR or TAVR as part of the PARTNER 1 and PARTNER 2 trials. Overall there were 107 cases of PVE from 8530 patients over a mean follow-up of 2.69±1.55 years. There was no significant difference between the incidence of TAVR-PVE and SAVR-PVE (5.21 vs. 4.10 PVE per 1000 person years, respectively, p=0.44). There was also no significant difference with regard to the temporal incidence of PVE between devices, with most infections occurring in the intermediate timeframe (30 days to 1 year). Independent predictors of PVE included baseline cirrhosis, renal insufficiency, and pulmonary disease. Interestingly, staphylococcus was more commonly the responsible organism in SAVR-PVE (58.3% vs 28.4% for TAVR-PVE) while streptococcus was more common in TAVR-PVE (28.4% vs 8.3% for SAVR-PVE).
Takeaway: The risk of PVE after TAVR and SAVR is low, with no difference in the predictors, temporal incidence, or overall incidence of PVE between devices.
Cardiac Surgery
Summarised by Dr David Bell
Intraoperative autologous blood donation (IAD), also known as acute normovolaemic haemodilution, is currently graded as a level IIB recommendation because of the lack of high-quality evidence. The aim of this study was to evaluate the effect of a blood conservation protocol focussing on IAD use in cardiac surgery. Over 8 years 1,002 patients were studied. 352 patients (group 1) were compared with 650 patients after the change in protocol (group 2). Propensity score matching was used to account for population differences. Fewer group 2 patients required blood transfusions during their hospital stay (78% vs 61%), they experienced a shorter length of stay (8.02 vs 7.28 days) and fewer complications (29.5% vs 18.8%). There was no difference in mortality.
Takeaway: IAD use is associated with reduced transfusions in cardiac surgery and should be considered a complementary aspect of blood conservation.
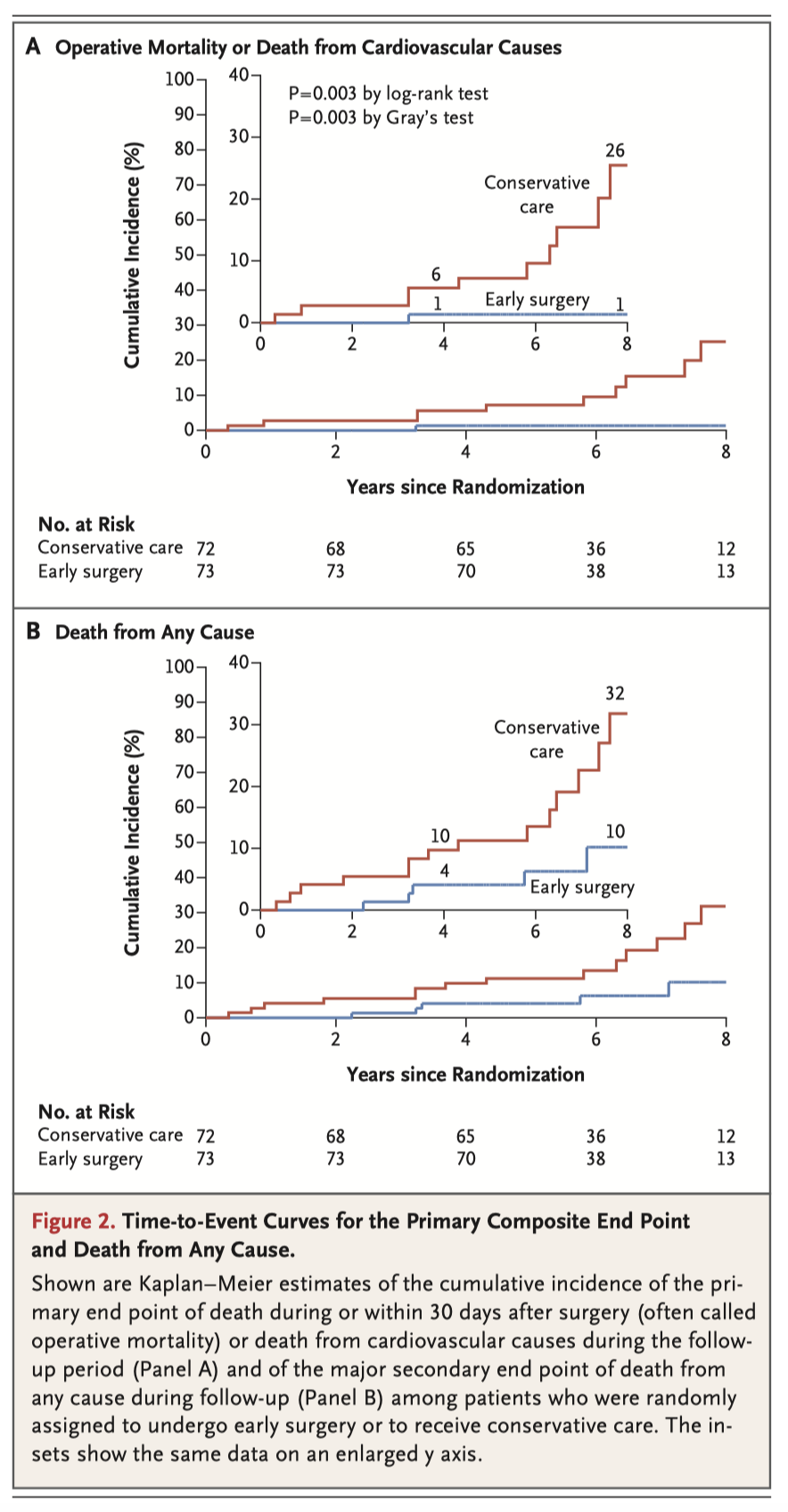
This small but significant study highlights both the short- and long-term consequences of delayed intervention in patients with asymptomatic severe AS. 145 patients with very severe AS were randomised to either early SAVR or to conservative care according to the recommendations of current guidelines. In an intention-to-treat analysis, the primary end point of either 30-day mortality or death from cardiovascular causes during follow up, occurred in 1/69 patients assigned to SAVR and 11/72 patients in the conservative-care group. Death from any cause occurred in 5 patients in the early SAVR group (7%) and in 15 patients in the conservative-care group (21%).
Takeaway: Patients with severe AS require early intervention.
Clinical implications: Either expansion of resources for TAVI programs should be provided, or TAVI risk assessment must take into account the significant mortality associated with long waiting times and early SAVR recommended instead.
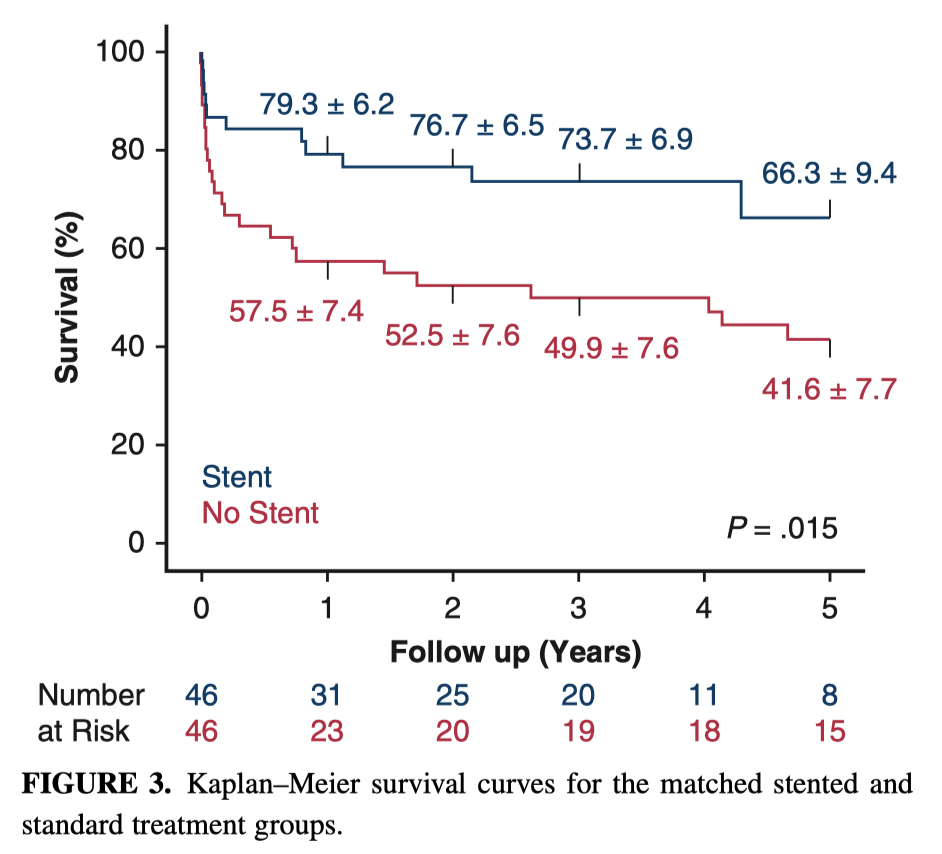
This study set out to determine the effect of antegrade stent delivery in the descending thoracic aorta on short- and mid-term clinical and imaging outcomes for patients who presented with a Type A dissection. In 178 propensity matched patients, insertion of an antegrade stent in patients with extension of the dissection in the false lumen resulted in improved short and mid-term survival, greater rates of aortic remodelling and fewer subsequent procedures. The 3- and 5-year survivals were 73.3% and 49.9% in the stented group and 66.3% and 41.6% in the standard group.
Takeaway: antegrade stent delivery at the time of a Type A Dissection improves short and mid-term mortality, rates of subsequent procedures term mortality. Results are inconclusive for spinal cord ischaemia.
Cardiac Imaging
Summarised by Dr David Bell
Severity of stenotic lesions is often determined by Doppler pressure gradients (DPG) as a surrogate for a catheter determined gradient. However suboptimal agreement between Doppler and catheter gradients exists. This study examined the occurrence of clinically significant recovered pressure (RP) in AS, PS, and CoA by assessing simultaneous DPG and catheter peak-to-peak gradient (PPG) in 82 patients both before and after correcting for RP. RP was calculated from a fluid dynamic–based equation. Recovered pressure corrected Doppler peak instantaneous gradient (PIG) had significantly closer agreement and correlation with the catheter PPG than the uncorrected PIG and mean Doppler gradients.
Takeaway: Significant RP occurs in congenital AS, PS, and CoA, accounting for misclassification of lesion severity by Doppler PIG. The RP magnitude is at a maximum in mild to moderate stenotic outflow lesions, with small-size downstream vessels causing the most misclassification of lesion severity by Doppler PIG.
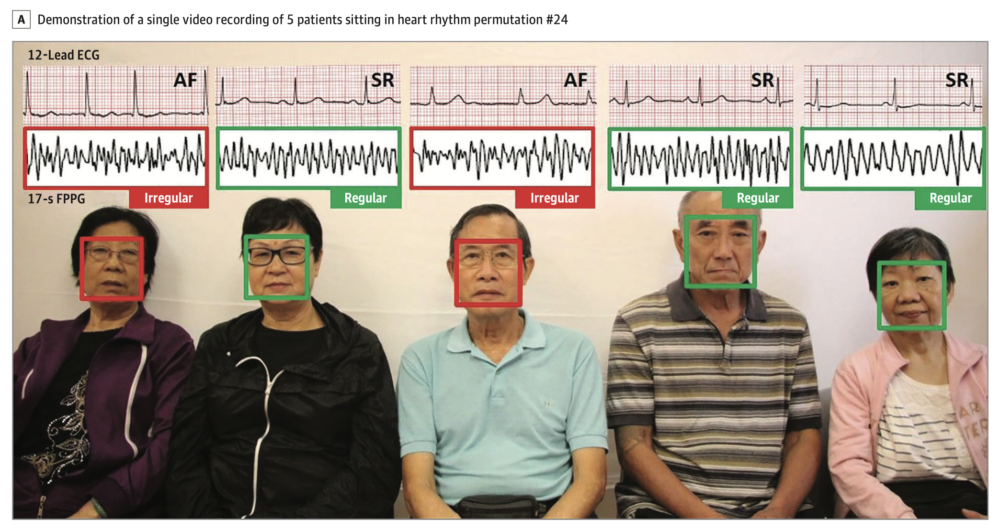
In 2018 this group demonstrated a novel method of AF detection using a smartphone camera. It required no physical contact but instead analysed facial photoplethysmography (FPPG). This study examines the feasibility of high-throughput AF detection by analysing FPPG signals from multiple patients concurrently using a single digital camera and a pretrained deep convolutional neural network (DCNN). 20 patients with permanent AF and 24 control individuals in sinus rhythm (SR) were recorded in randomly assigned groups of 5 across 64 videos of 1-minute duration. The FPPG signals from patients were automatically extracted from the videos, with pulse irregularity in more than 50% FPPG segments for each patient considered positive for AF. A total of 320 individual FPPG signals were analysed. Agreement between the camera phone FPPG and ECG occurred in just under 96% of cases.
Takeaway: mass screening of AF using FPPG in concurrent patients performs well already.
Clinical implications: this is the first study to demonstrate detection of AF with high accuracy from multiple patients concurrently with a single camera. This raises the possibility that this low-cost approach may be scalable for high-throughput AF screening. Further studies are warranted to evaluate performance in a real-world clinical and home setting.
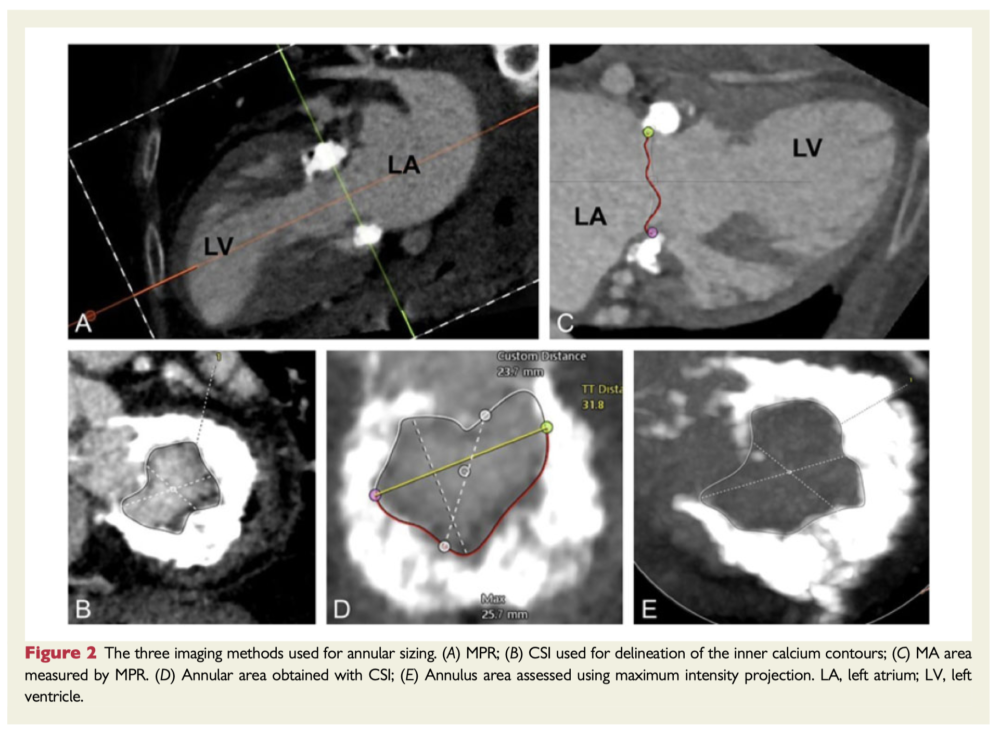
The aim of this study was to investigate valve sizing and the haemodynamic relevance of the predicted left ventricular outflow tract (LVOT) in patients with mitral annular calcification (MAC) undergoing transatrial transcatheter valve implantation (THV). 21 patients undergoing transatrial THV underwent multiplanar reconstruction (MPR), maximum intensity projection (MIP), and cubic spline interpolation (CSI) were compared for MA sizing during diastole. In addition, predicted neo-LVOT areas were measured in 18 patients and correlated with the post-procedural haemodynamic dimensions. Sizing using MPR and MIP yielded comparable results in terms of area, perimeter, and diameter, whereas the dimensions obtained with CSI were systematically smaller.
Takeaway: In patients with severe MAC undergoing transatrial transcatheter valve implantation, MPR, and MIP yielded comparable annular dimensions, while values obtained with CSI tended to be systematically smaller. Mitral annular area and the average annular diameter seem to be the most reliable parameters for valve selection. Simulated relative LVOT reduction was found to predict the post-procedural aortic gradients.
Perioperative Medicine
Summarised by Dr Andrew Haymet
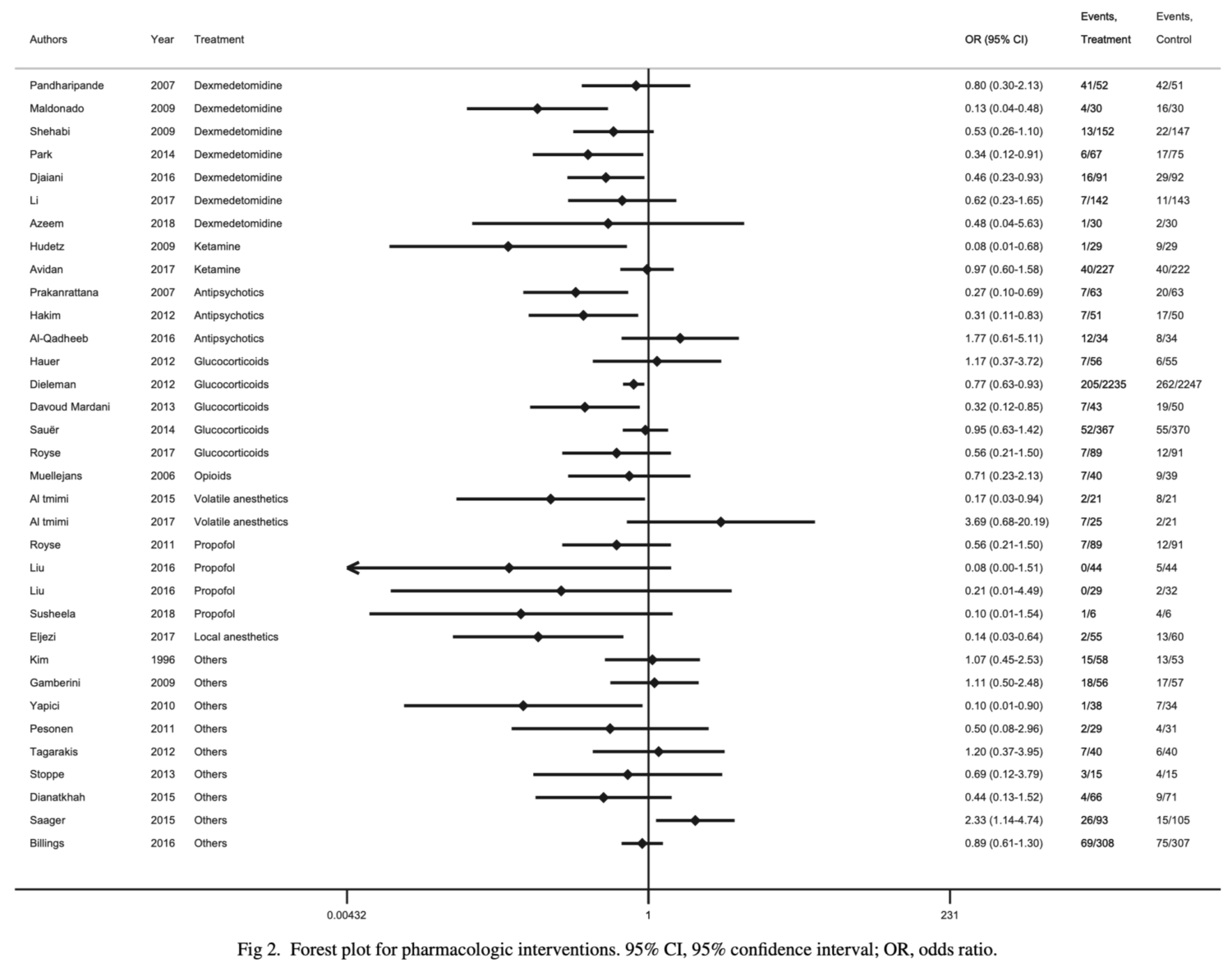
Postoperative delirium after cardiac surgery is associated with prolonged hospital admissions and increased mortality. This systematic review included 56 studies up until July 2018, of which 91% focused on prevention of delirium and 9% on its management. The most frequently analyzed strategies were the administration of dexmedetomidine, ketamine, antipsychotics, glucocorticoids, propofol, opioids, volatile and local anaesthetics, and remote ischaemic preconditioning. Of these strategies, the authors concluded that dexmedetomidine was the most frequently studied agent, and that it might reduce the occurrence of delirium after cardiac surgery.
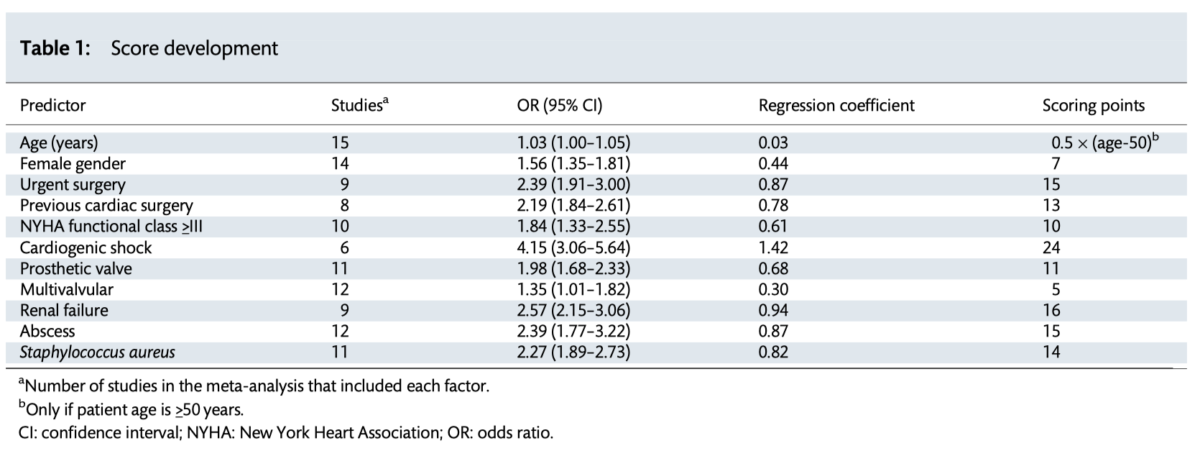
There are well validated risk prediction models for general valve surgery, however few specifically developed for infective endocarditis or validated in this population. In this study, the prognostic utility of a new score (APORTEI) was evaluated using patient-level data from a multicentric national cohort. Patients who underwent surgery between 2008 and 2018 were included. The APORTEI score was calculated in 1338 patients, based on eleven variables, with an observed surgical mortality rate of 25.56%. The authors concluded that the APORTEI score showed an adequate estimation of the risk of mortality after surgery for IE in a nationwide cohort.
This special article synthesizes research highlights of 2019 in cardiac and vascular anaesthesia. Five major themes are described, including updates in transcatheter aortic and mitral valve replacement, left ventricular assist devices with an emphasis on the Heartmate 3 device, coronary artery bypass grafting with emphasis on robotic surgery and conduit selection, pulmonary hypertension and associated outcomes in noncardiac surgery, and finally the use of volatile anaesthetics versus total intravenous anaesthesia for cardiac surgery.




