Welcome to the monthly SHDA Research Update. Our specialists have selected 3 seminal papers that have been recently published in each speciality (Cardiology, Cardiac Surgery, Cardiac Imaging, Perioperative Medicine).
Cardiology
Summarised by Dr Sarah Catchpoole
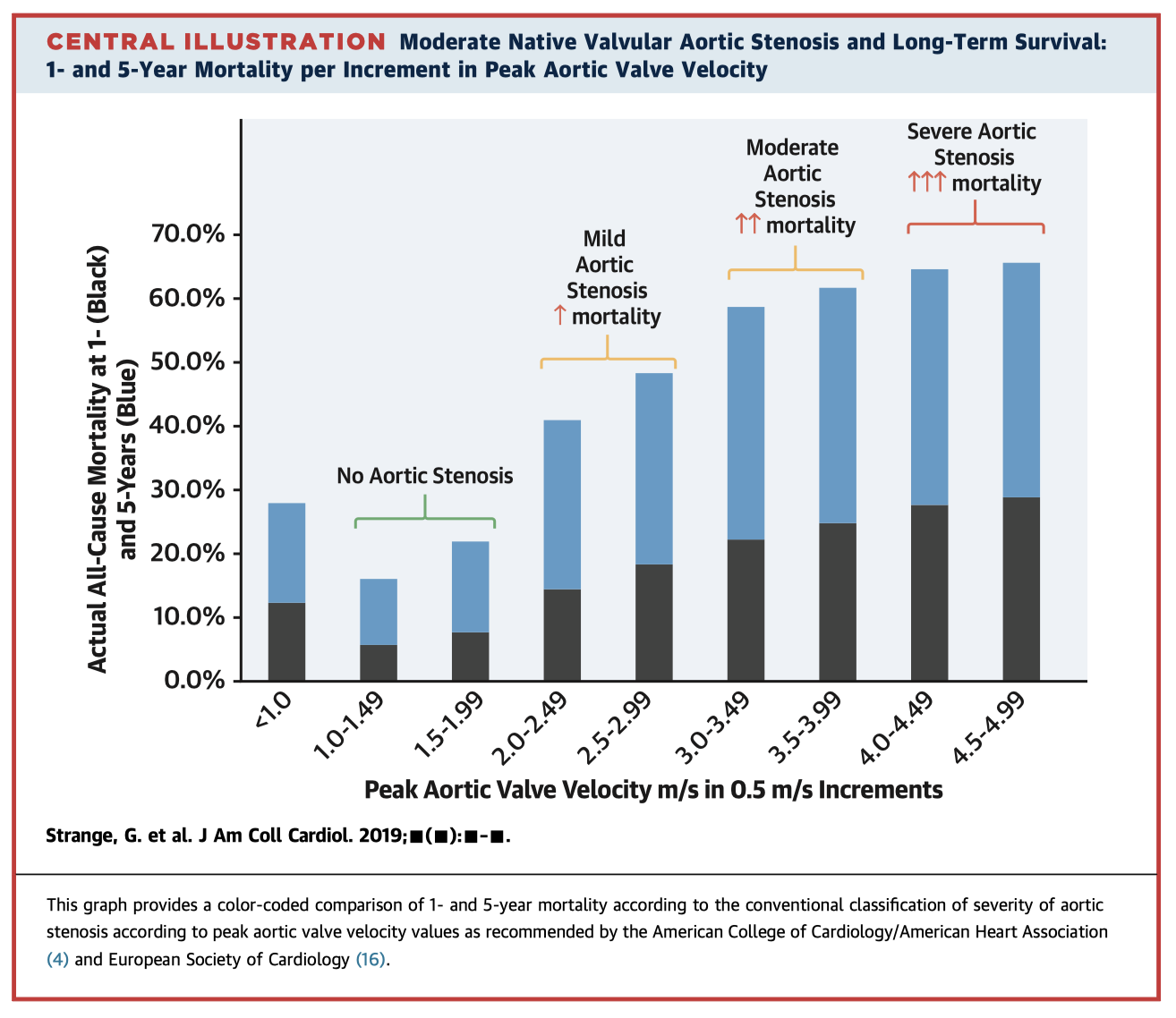
This large observational study substantially adds to our understanding of the natural history of AS. Using the National Echocardiographic Database of Australia, the authors identified 241,303 eligible individuals of which 16,129 had mild AS; 3,315 moderate AS; and 6,383 severe AS. Patients were followed up for a median of 1,208 days. The key finding was that even moderate AS was associated with poor long-term survival (5-year mortality 56%, compared to 67% for severe AS). The authors suggest these findings should spur re-evaluation of the traditional conception of moderate AS as a benign condition, and the potential benefit of earlier therapeutic intervention.
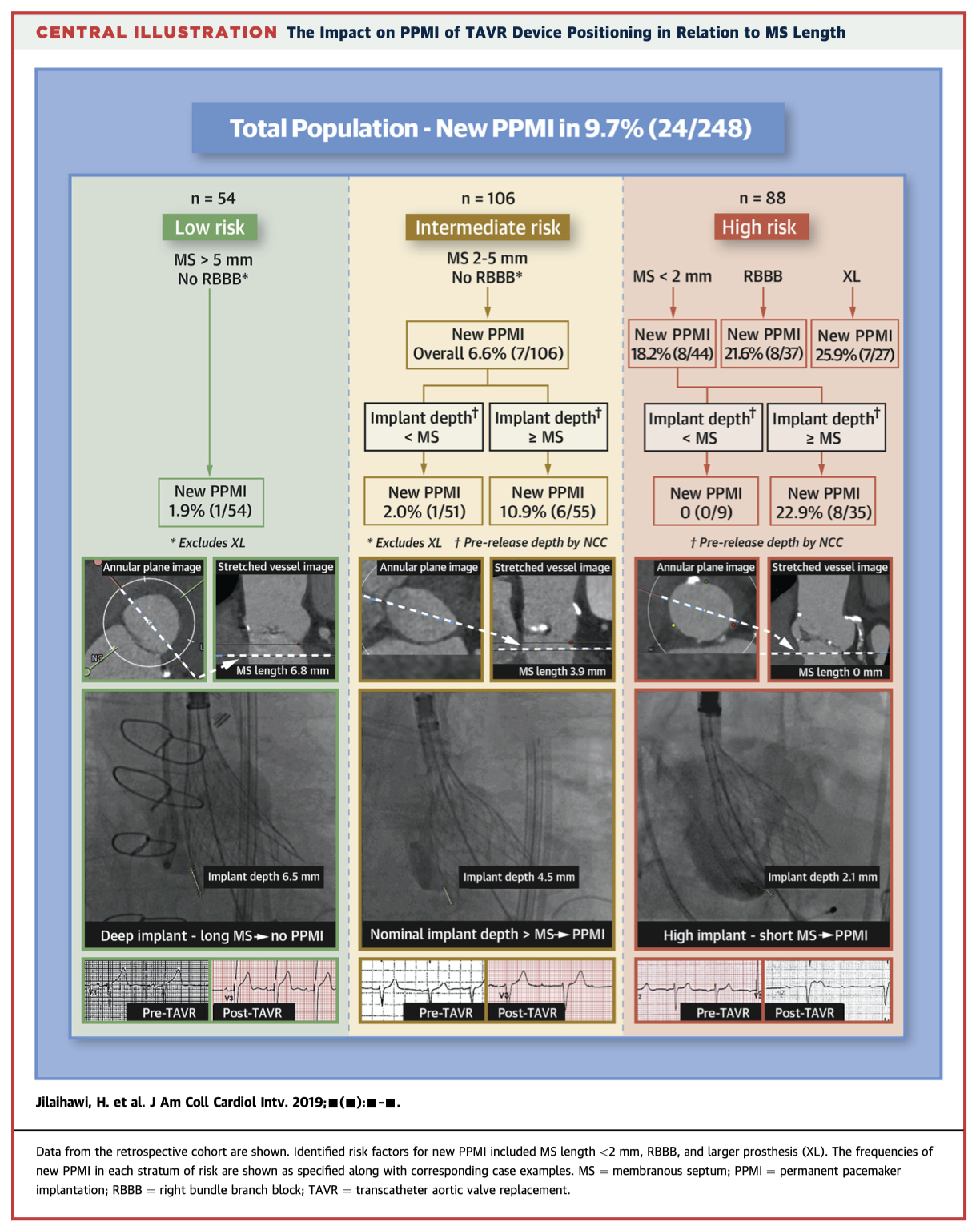
Permanent pacemaker (PPM) implantation is a known complication of TAVR. In a retrospective analysis of 248 patients, the authors found that implant depth greater than the length of the membranous septum was an independent predictor of PPM implantation (OR 8.04, p<0.001). In a subsequent prospective series of 100 patients, proceduralists used a repositionable self-expanding device with the aim to implant at minimum depth from the membranous septum (MIDAS approach). This significantly reduced the rate of PPM implantation (3.0% compared to 9.7%, p=0.035) and the rate of new left bundle branch block (9% compared to 25.8%, p<0.001).
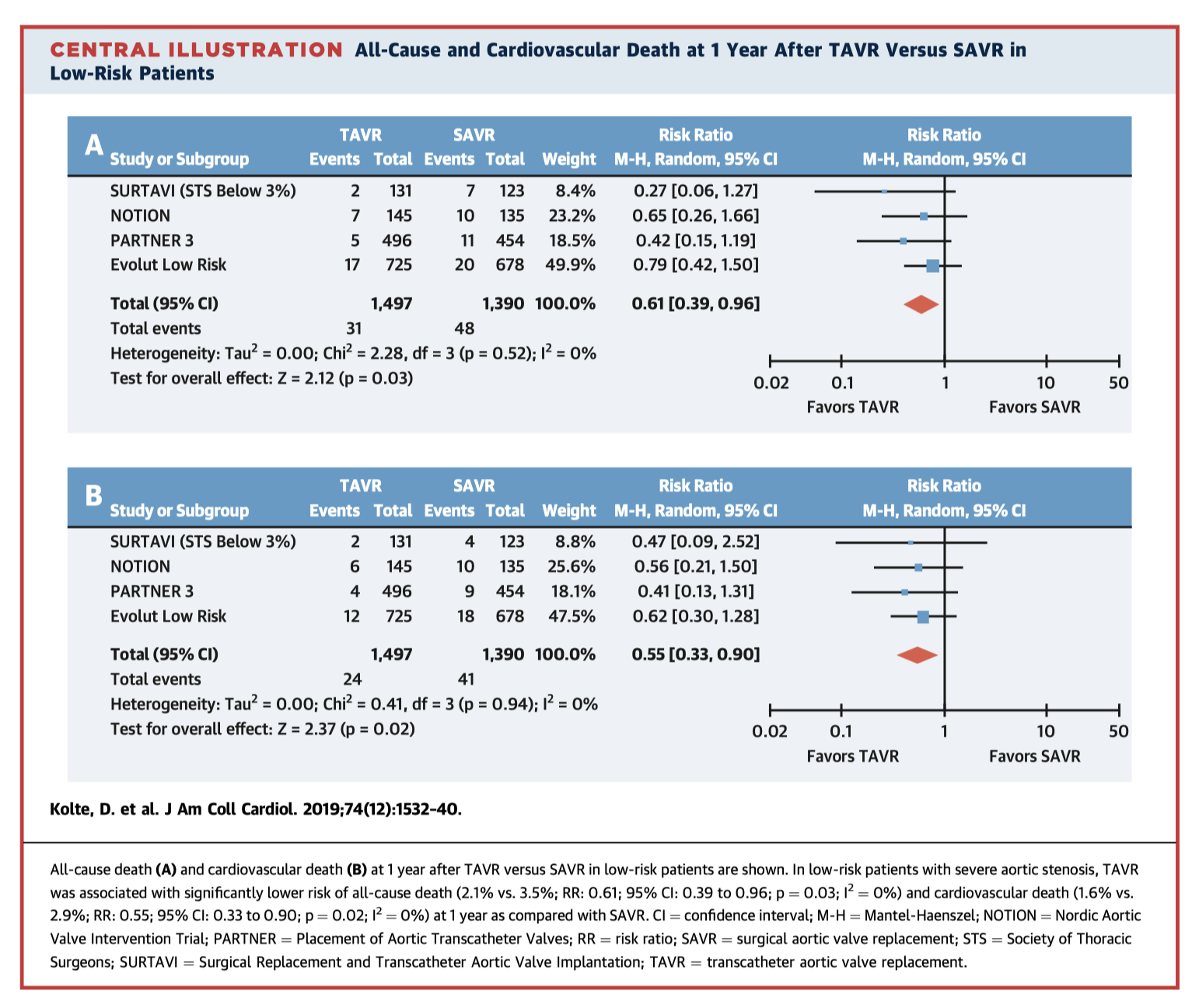
This the first meta-analysis to compare TAVR vs SAVR in low-risk patients with severe AS. Data were available for 2,887 patients (1,497 TAVR; 1,390 SAVR) across four RCTs. Overall, TAVR was associated with significantly lower all-cause and cardiovascular mortality at 1 year. In terms of procedural complications, TAVR had lower rates of severe bleeding, worsening atrial fibrillation, and acute kidney injury; but higher rates of PPM implantation and moderate-severe paravalvular leak. The findings suggest that TAVR is appropriate in low-risk patients, however the long-term outcomes in this population are still not known.
Cardiac Surgery
Summarised by Dr Andrew Haymet
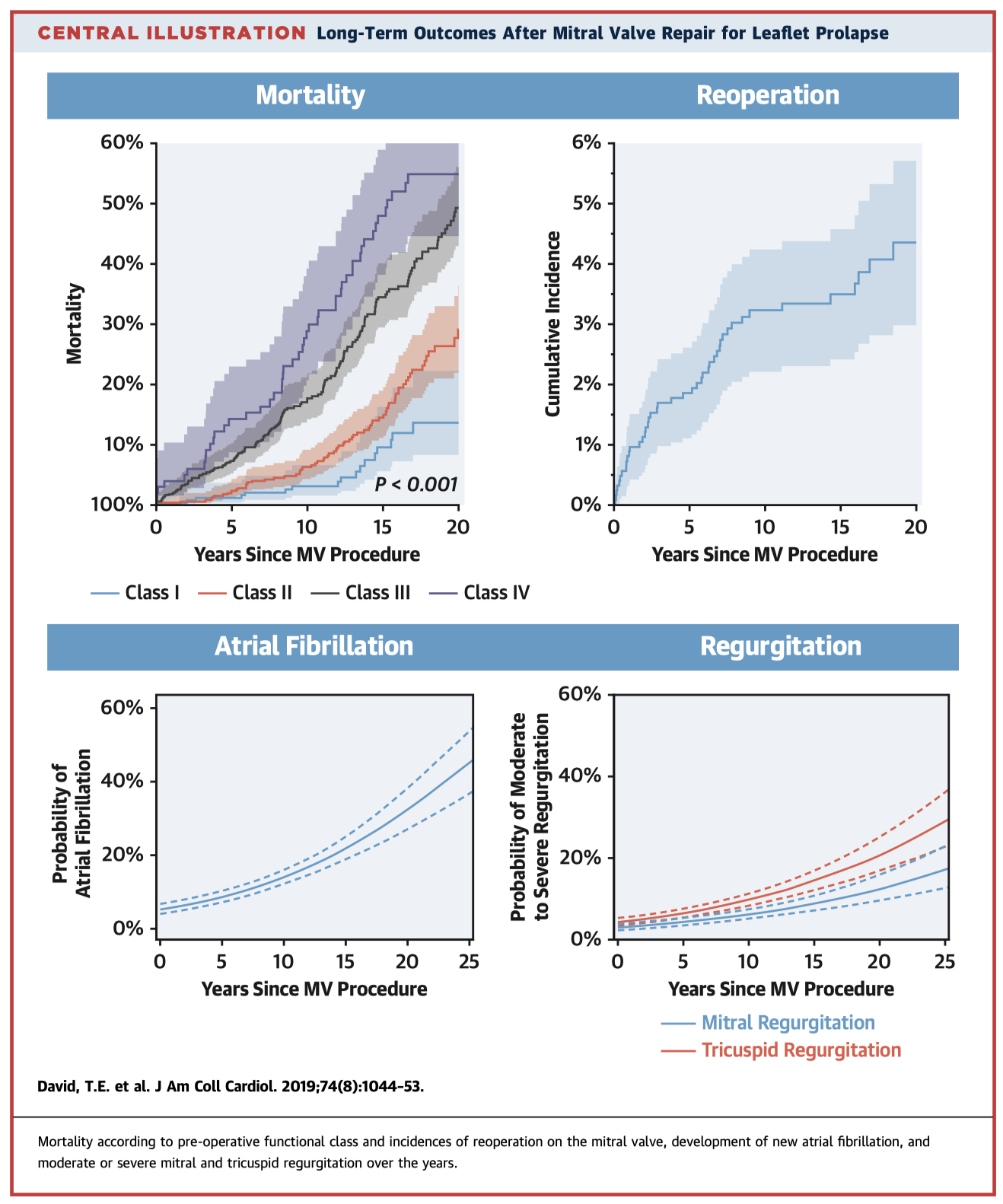
Mitral valve (MV) repair has become first line therapy for mitral regurgitation (MR) secondary to degenerative disease, however there are limited data regarding late outcomes. In this study of 1,234 consecutive patients who underwent MV repair for leaflet prolapse, 20-year reoperation-free survival was 60.4% (95% CI, 56.2-64.2%). Risk factors associated with recurrent MR were older age, complete heart block, MV repair without annuloplasty ring, and degree of myxomatous change of the MV. The authors concluded that MV reoperation was uncommon following MV repair, however there was an increasing incidence of recurrent MR, TR, and new AF over time.
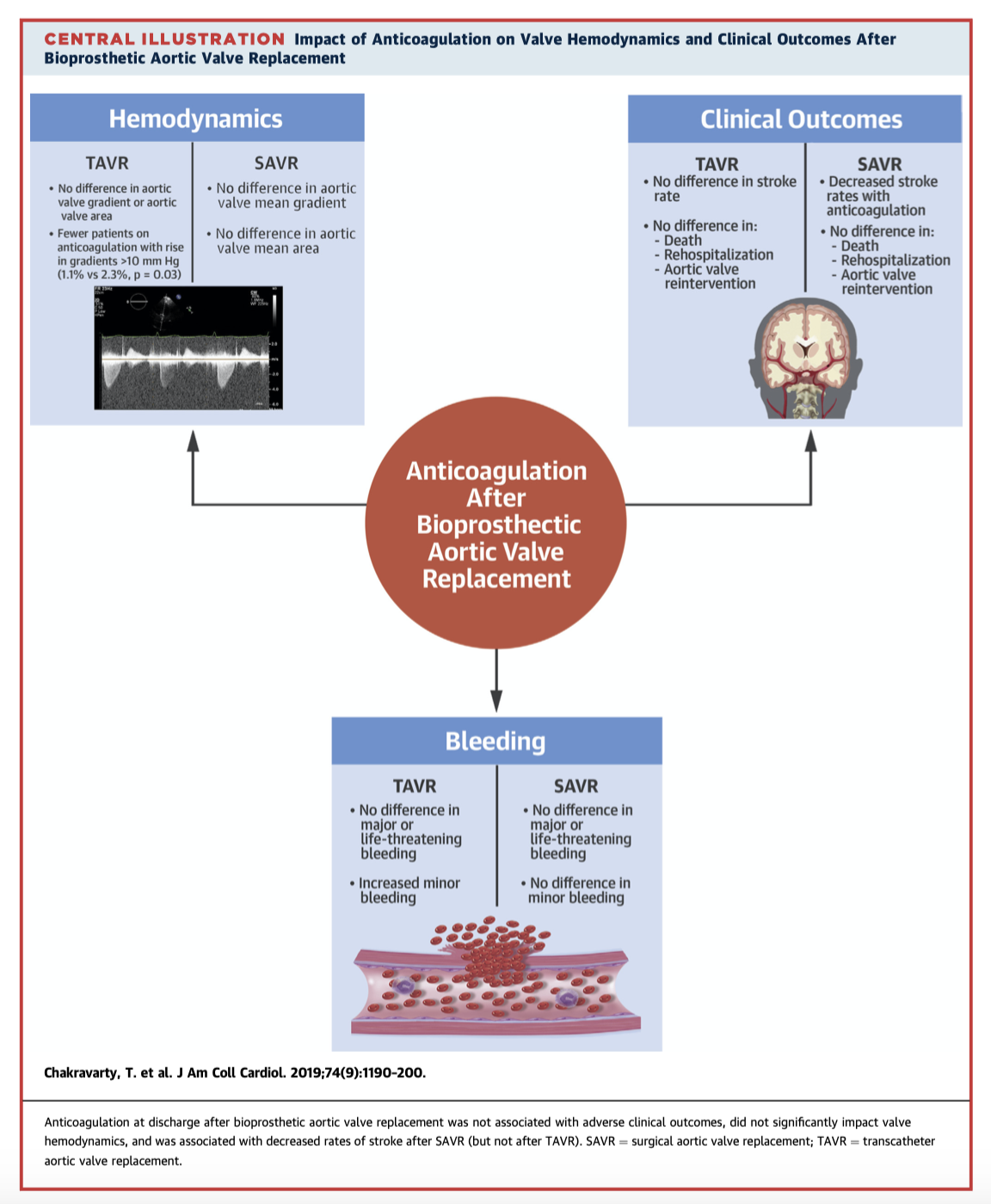
There are limited data regarding the effect of anticoagulation on valve haemodynamics and outcomes following bioprosthetic AVR. In this study of 4,832 patients who received either TAVR (n=3,889) or SAVR (n=943), early anticoagulation in the short term did not result in more adverse clinical events; did not significantly affect valve haemodynamics; and was associated with lower rates of stroke after SAVR, but not after TAVR. Further studies are required to ascertain the effect of early anticoagulation after bioprosthetic AVR on long term outcomes.
There are limited data regarding long term pulmonary valve function following the Ross procedure. This study retrospectively reviewed 443 patients who underwent the Ross procedure using a cryopreserved pulmonary allograft. At 5, 10, 15 and 20 years excellent long term function was shown, with infrequent significant pulmonary allograft dysfunction found. Reintervention was only rarely indicated for infective endocarditis, severe pulmonary stenosis, and severe pulmonary regurgitation.
Cardiac Imaging
Summarised by Dr Sarah Catchpoole
3D Echocardiography is a useful real-time adjunct to traditional 2D imaging. This state-of-the-art review focuses on areas where 3D echo could be of most benefit in routine clinical practice. The authors recommend all patients should undergo focused examination of left ventricular volume, left ventricular ejection fraction, and global longitudinal strain. In the setting of cardiac pathology, 3D echo is most useful for the assessment of mitral valve pathologies, atrial septal defects, and for peri-procedural planning.
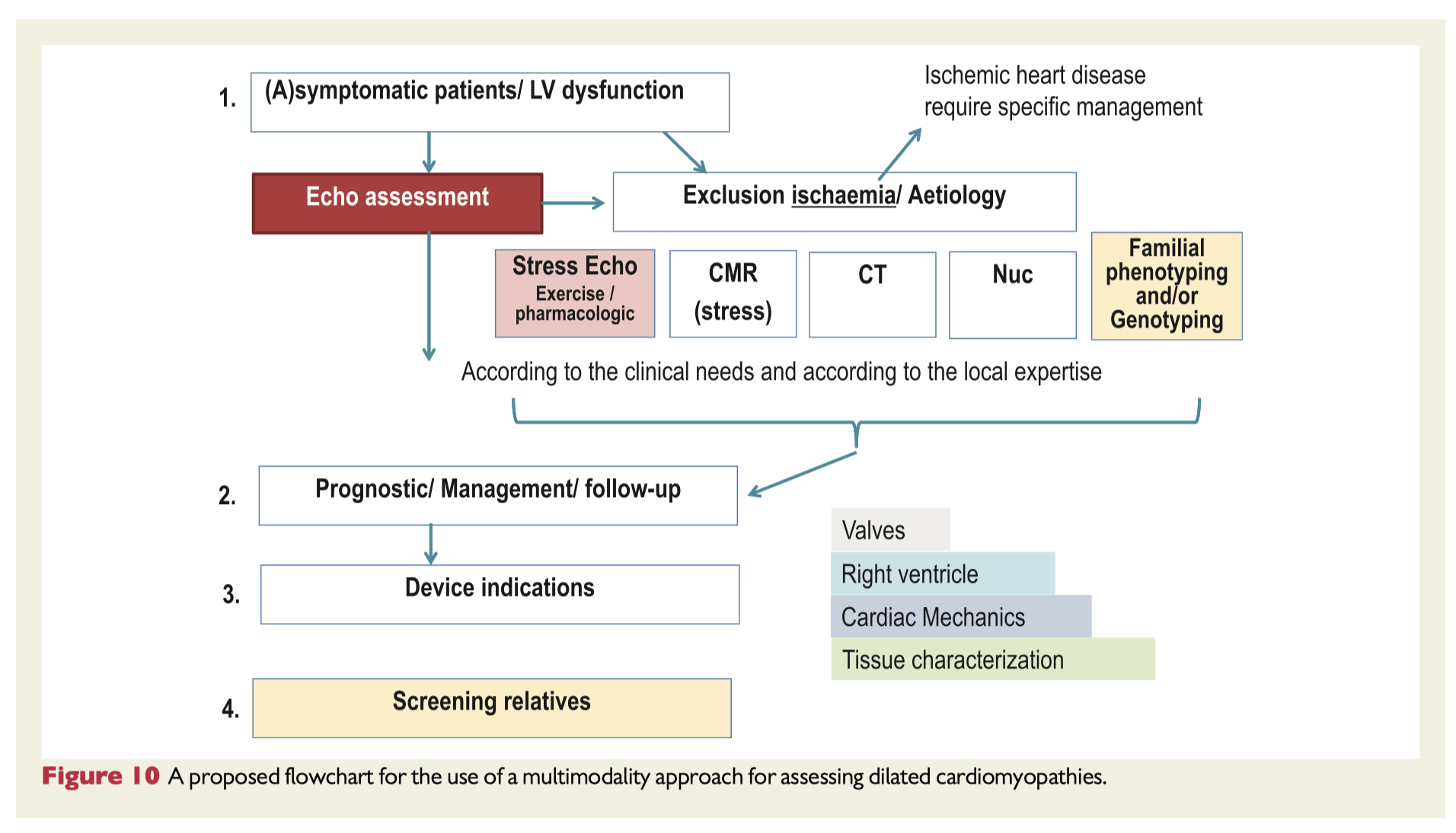
Dilated cardiomyopathy (DCM) is a heterogenous disease which relies heavily on imaging for diagnosis, prognosis and management. However, there is little guidance regarding multimodality imaging in DCM. This expert consensus document briefly reviews the clinical spectrum and diagnostic criteria for DCM, before covering imaging options in detail with a focus their utility in clinical practice to address specific patient scenarios. The recommendations are summarised in a 13 point document. The authors stress that imaging techniques should be used selectively to answer a particular clinical question, and that all imaging techniques need not be repeated in all DCM patients.
Perioperative Medicine
Summarised by Dr Andrew Haymet
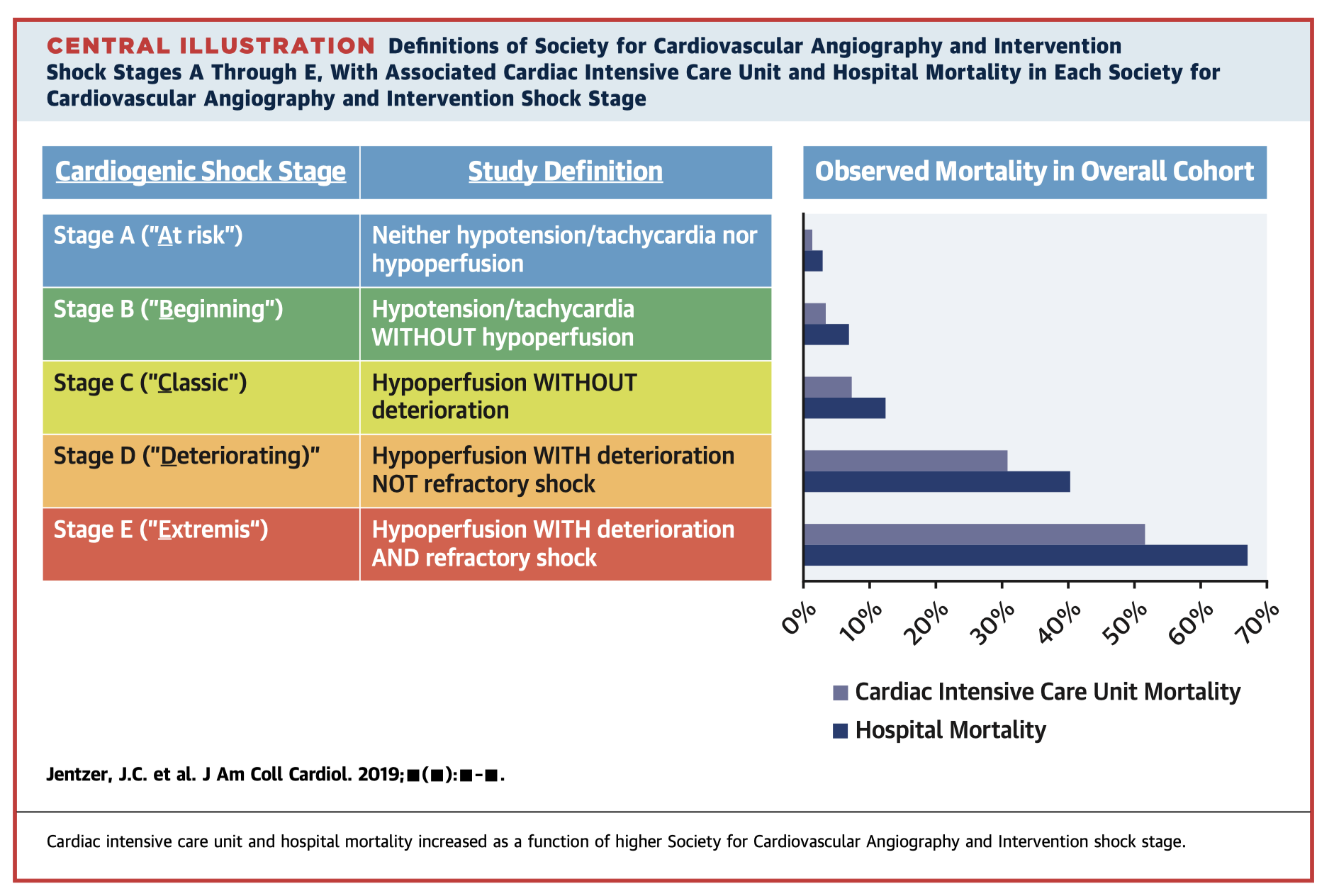
This retrospective analysis of 10,004 patients reviewed a new 5-stage system for classifying cardiogenic shock from the Society for Cardiovascular Angiography and Intervention (SCAI). After multivariable adjustment, each higher SCAI shock stage was associated with increased hospital mortality. This classification system provided sound hospital mortality risk stratification, and could therefore potentially be used to identify and predict mortality risk in patients with, and at risk of, cardiogenic shock.
Bivalirudin is a direct thrombin inhibitor with both a short onset of action and half-life and is an alternative anticoagulant to a heparin/protamine regimen. Its mechanism of action includes inhibition of plasma thrombin, clot bound thrombin, and collagen induced platelet activation. This may confer superiority over heparin by mitigating the postoperative prothrombotic state and therefore positively affecting early coronary graft patency following off-pump coronary bypass grafting. Its application in cardiac surgery using cardiopulmonary bypass (CPB) has been limited due to the superiority of heparin in terms of cost, ease of monitoring, and availability of its reversal agent, protamine. Key points for successful use of bivalirudin during CPB are avoidance of blood stasis, and meticulous perioperative medical management. Further studies are required to better ascertain applications for this therapy.
This prospective observational study of 30 patients with normal myocardial function tested the hypothesis that longitudinal strain of the right ventricle (RV) is significantly reduced in patients undergoing cardiac surgery with extracorporeal circulation and cardioplegic arrest at the end of surgery, with RV ejection fraction remaining constant. In these patients, longitudinal contraction of the RV lateral and inferior wall, the RV outflow tract, and the interventricular septum was found to be impaired postoperatively, and was compensated for by an increase in circumferential contraction without changes in RV ejection fraction.