Welcome to the monthly SHDA Research Update. Our specialists have selected 3 seminal papers that have been recently published in each speciality (Cardiology, Cardiac Surgery, Cardiac Imaging, Perioperative Medicine).
Cardiology
Summarised by Sarah Catchpoole
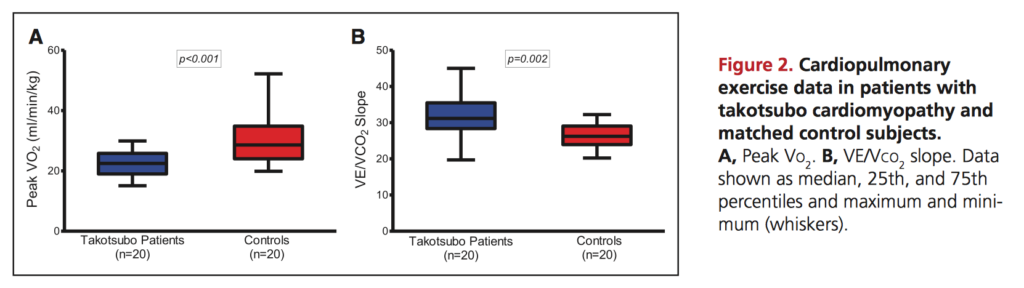
This study challenges the common perception that Takasubo cardiomyopathy is a self-limiting condition. Rather, the authors found persisting impairments, all consistent with a long-term heart failure phenotype. Of 37 patients with a prior diagnosis of Takasubo cardiomyopathy (minimum >12 months, range 13–39, median 20), 88% reported persistent symptoms consistent with heart failure (Minnesota Living with Heart Failure Questionnaire), predominantly due to physical rather than emotional symptoms. Consistent with this, subjects had poorer exercise tolerance – only 54% were able to exercise to the required RER of 1.1 and overall they had reduced peak oxygen consumption and increased VE/VCO2 slope compared with matched controls (Figure 2, below). Functional imaging demonstrated ongoing cardiac dysfunction, including reduced global longitudinal strain (p=0.006) and impaired cardiac energetic status (phosphocreatine/γ-adenosine triphosphate ratio). The authors recommend patients with Takasubo be counselled regarding potential longer-term symptomatic limitations and urge further studies to investigate the mechanism of ongoing cardiac dysfunction.
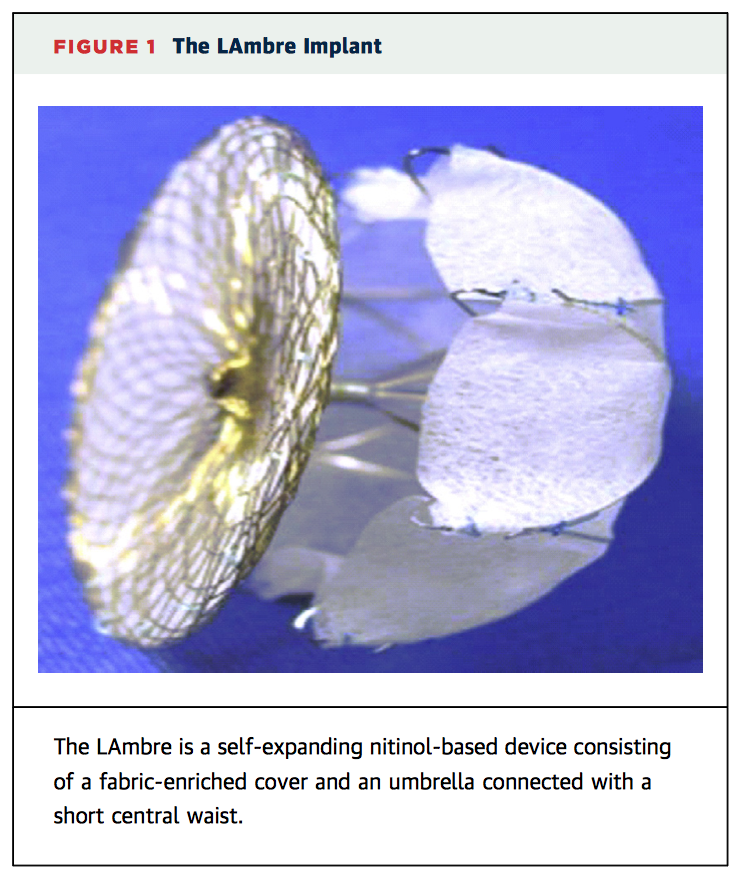
Cardioembolic stroke is a common complication of atrial fibrillation (AF), with more than 90% of thrombi found in the left atrial appendage (LAA). This is the first-in-human pilot trial of the new LAmbre self-expanding LAA occlusion device (Lifetech Scientific, Shenzhen, China). The device (Figure 1, below) is implanted percutaneously via the transeptal route. Across 12 centres, 153 patients with non-valvular AF, unsuitable for long-term anticoagulation with warfarin, and a minimum CHADS2 score of 1 were prospectively enrolled. 152 had the device successfully implanted (99.4%), with 5 serious complications (3.3%), including serious pericardial effusion (n=3), ischaemic stroke (n=1), and major bleeding (n=1). There were no cases of device embolisation post-operatively or at 12 month follow up. Other results at 12 months are summarised in Table 4, below. Of note, 99% of patients maintained good LAA seal with >3mm residual flow. There were 2 cases of thrombus formation on the device, and 2 cases of ischaemic stroke (1.3%, for both). Overall, the authors conclude the LAmbre device shows encouraging results.
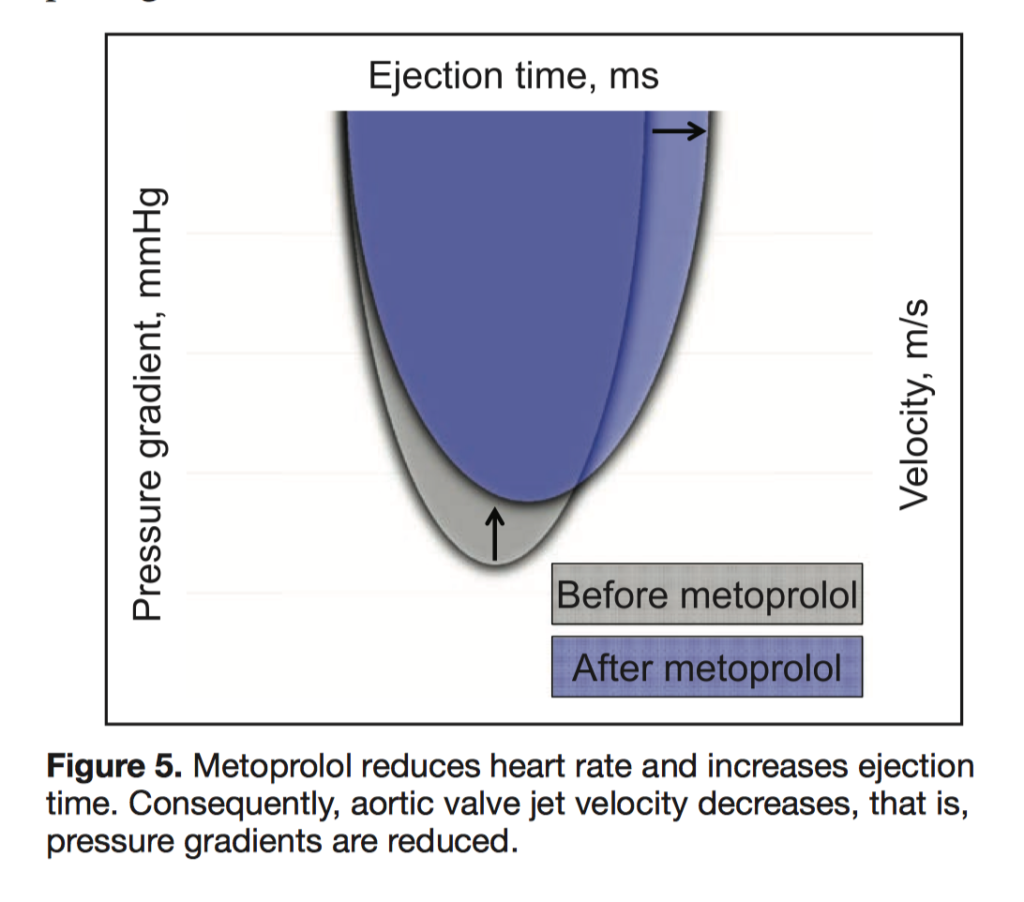
This is the first randomised, double-blinded trial to investigate the effect of metoprolol in patients with aortic stenosis (AS), and to prospectively demonstrate that beta blockers may alter the natural history of the disease. 40 patients with asymptomatic AS received either placebo or metoprolol (50–200mg once daily, titrated individually) for a treatment period of 22 weeks. Metoprolol was found to significantly decrease heart rate (p=0.003), prolong ejection time (p=0.03) and therefore decrease aortic valve gradients and valvuloarterial impedance (-11%, p=0.03) compared with placebo. In terms of metabolic effects, myocardial oxygen consumption (MVO2) was significantly reduced by 12% (p=0.01). While longer trials are needed, the authors conclude metoprolol is safe and does induce short-term haemodynamic and metabolic changes, which may represent a breakthrough in the ongoing search for medical therapy effective in AS.
Cardiac Surgery
Summarised by Andrew Haymet
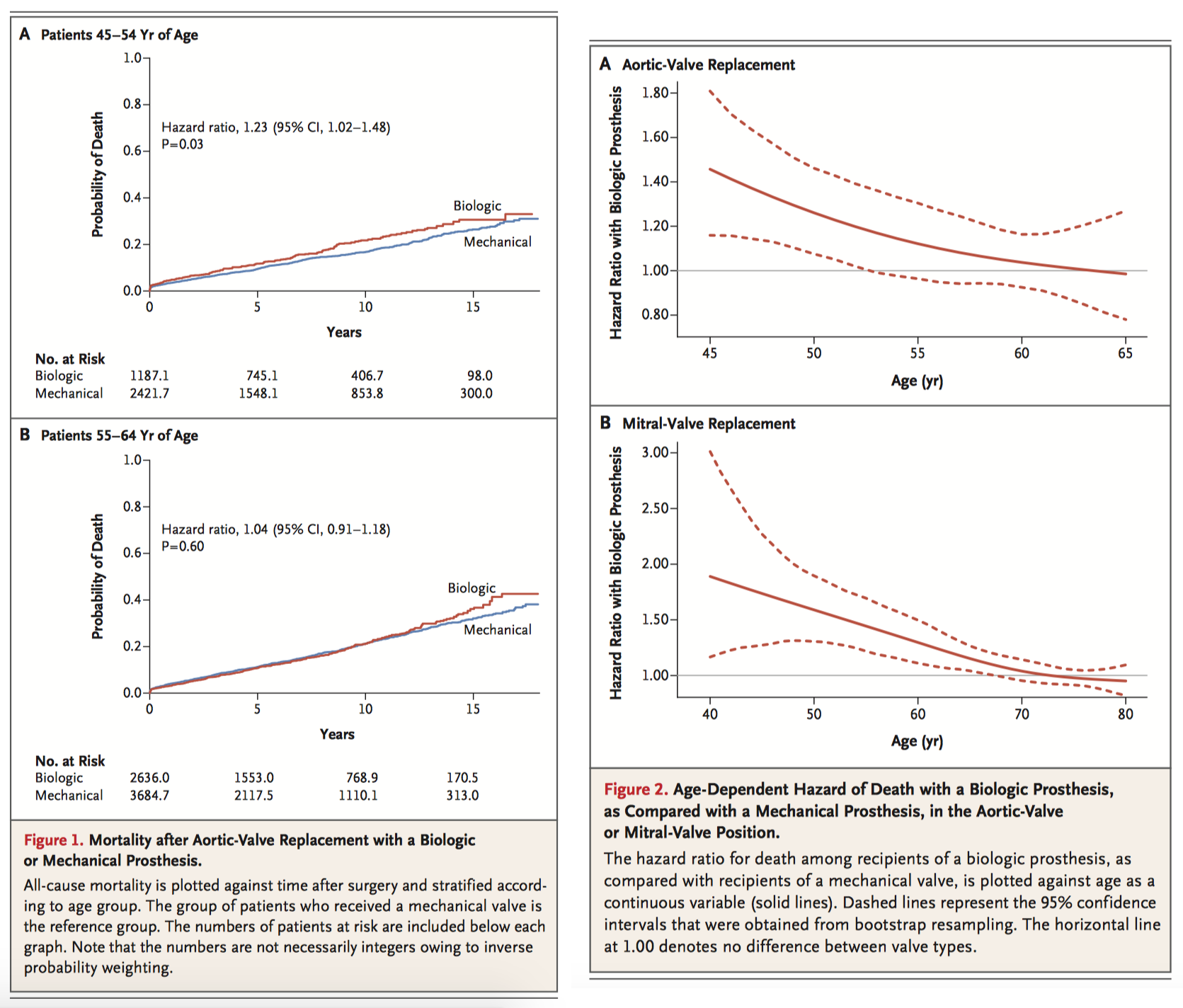
Aortic and mitral bioprosthetic valves have been increasingly favoured over mechanical valves despite limited evidence supporting this practice. This study compared long term mortality and rates of reoperation, stroke, and bleeding in patients who underwent primary aortic or mitral mechanical or bioprosthetic valve replacement between 1996 and 2013. For AVR, receipt of a biologic prosthesis was associated with a significantly higher 15 year mortality than receipt of a mechanical prosthesis in patients aged between 45 to 54 years, but not among those aged 55-64 years (30.6% vs. 26.4% at 15 years; hazard ratio, 1.23; 95% confidence interval [CI], 1.02 to 1.48; P = 0.03). For MVR, receipt of a biologic prosthesis was associated with significantly higher mortality than receipt of a mechanical prosthesis among patients 40 to 49 years of age (44.1% vs. 27.1%; hazard ratio, 1.88; 95% CI, 1.35 to 2.63; P<0.001) and among those 50 to 69 years of age (50.0% vs. 45.3%; hazard ratio, 1.16; 95% CI, 1.04 to 1.30; P = 0.01). The long term mortality benefit associated with a mechanical prosthesis compared to biologic persisted until 70 and 55 years of age in patients requiring MVR and AVR respectively.
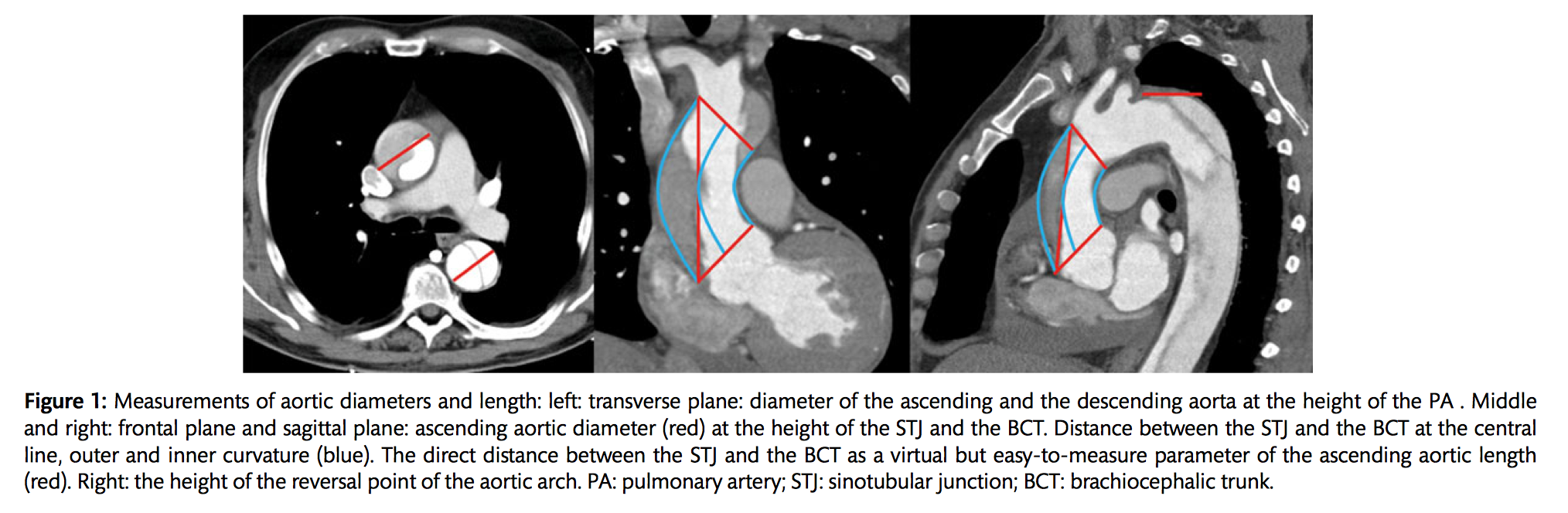
The role of ascending aortic elongation in the pathogenesis of Type A aortic dissection (TAD) is largely unclear. Clinical and computer tomography angiography (CTA) data were retrospectively reviewed and analysed from TAD patients (n=130), patients who developed a TAD later in their clinical course (preTAD, n=16) and healthy control patients who received a CTA for non-aortic emergencies (n= 165). The median ascending aortic diameter at the height of the pulmonary artery in TAD (50 mm) was significantly (P < 0.001) larger compared with the respective diameter of the healthy aortas (34mm). The midline length of the healthy ascending aortas was 71 mm. In the preTAD and TAD aortas, the same values were 81 mm and 92 mm, respectively (both P < 0.001). The authors concluded that aortic diameter might not be an optimal parameter to predict dissection, with most aortas dissecting at diameters below 55mm. Both the the TAD and preTAD aortas were elongated compared with the healthy controls. Therefore, aortic elongation may play a role in the pathogenesis of, and may be a risk factor for TAD.
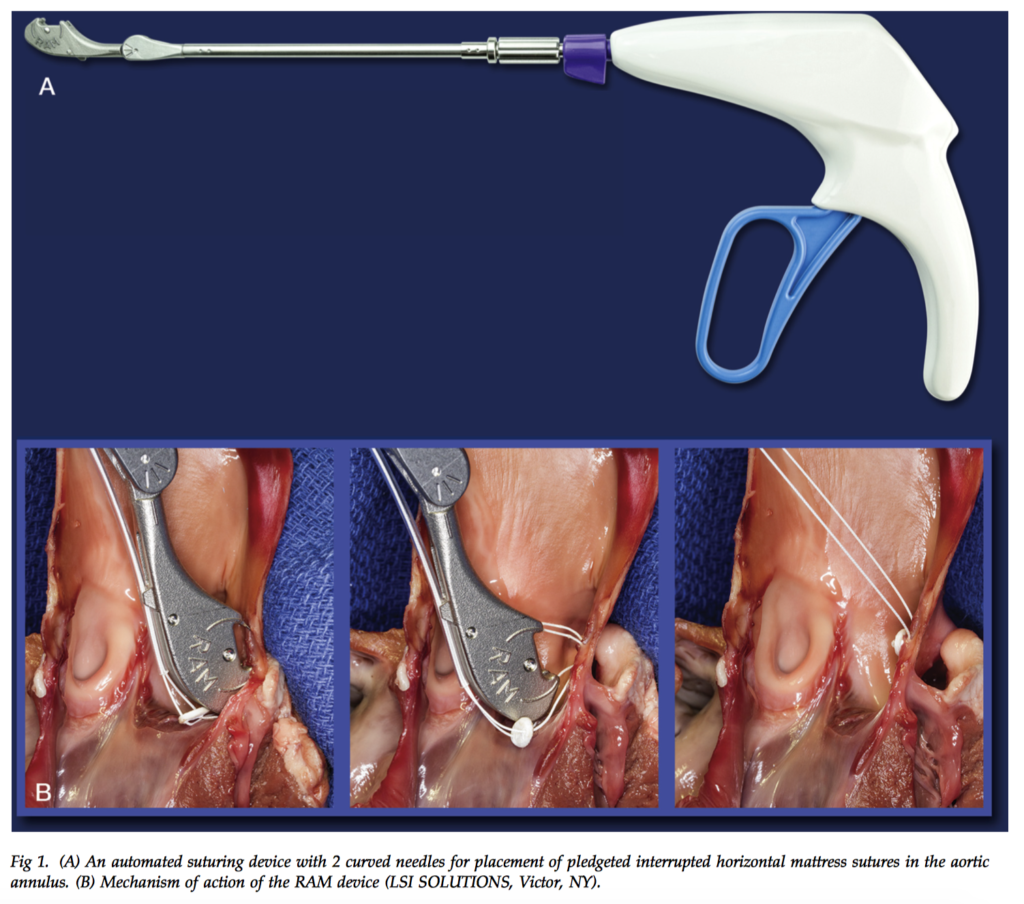
Annular suture placement during minimally invasive right anterior thoracotomy aortic valve replacements (MI-AVR) can be challenging. This study presented a novel automated suturing device which simultaneously drives dual-curved needles through the aortic annulus to place a pledgeted horizontal mattress suture remotely, whilst a second device with 2 straight needles places suture through the sewing cuff of a prosthetic heart valve. Automated annular suturing was successfully used in 5 MI-AVR cases, with no paravalvular leaks detected and a mean aortic valve gradient of 6.4mmHg postoperatively. All 5 patients were successfully discharged home following mean ICU and total length of stay of 2 and 7 days, respectively. The authors concluded that automated suturing during MI-AVRs is feasible and may reduce the technical challenge of this operation, however further studies are required to better ascertain patient outcomes.
Cardiac Imaging
Summarised by Sarah Catchpoole
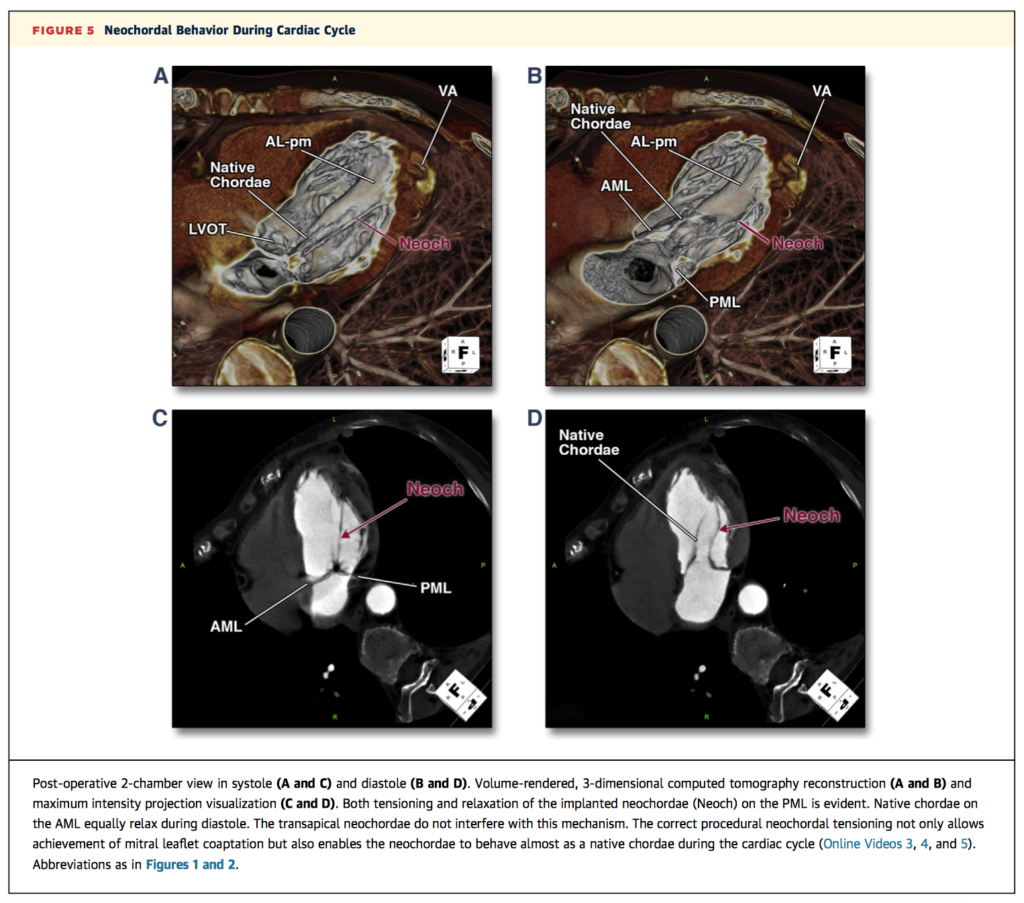
This brief imaging vignette demonstrates the use of CT for pre-operative guidance and post-operative assessment in transapical mitral valve repair with implantation of polytetrafluoroethylene neochordae. Example volume-rendered reconstructed images are provided for potential applications including selection of intercostal and ventricular access sites, planning trajectories of implanted neochordae, and post-operative evaluation, including dynamic behaviour of the neochardae during the cardiac cycle (Figure 5, below). Further online videos are available via the journal website.
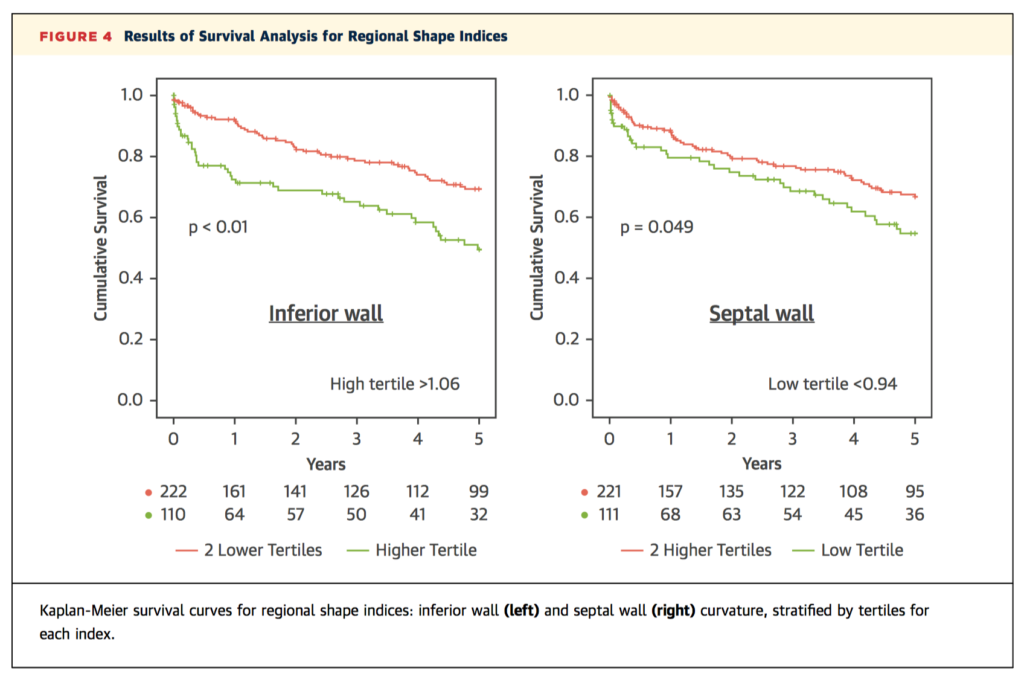
Both left ventricular ejection fraction (LVEF) and global longitudinal strain (GLS) derived from 2D echocardiography (2DE) have previously been found to predict mortality – could 3D echocardiography (3DE) add any prognostic value? This retrospective cohort study examined 416 inpatients referred for transthoracic echocardiography and followed up for a mean of 5±3 years. Cox regression revealed all four echocardiographic indices (2DE and 3DE LVEF and GLS) predicted cardiovascular mortality, with GLS overall superior to LVEF, and 3DE GLS the strongest overall predictor. In addition, inferior and septal wall curvature on 3DE, age, and body surface area were also independently associated. The authors note the restriction of the population to inpatients, with good quality images, in sinus rhythm, limits the generalisability of the findings to a broader population.
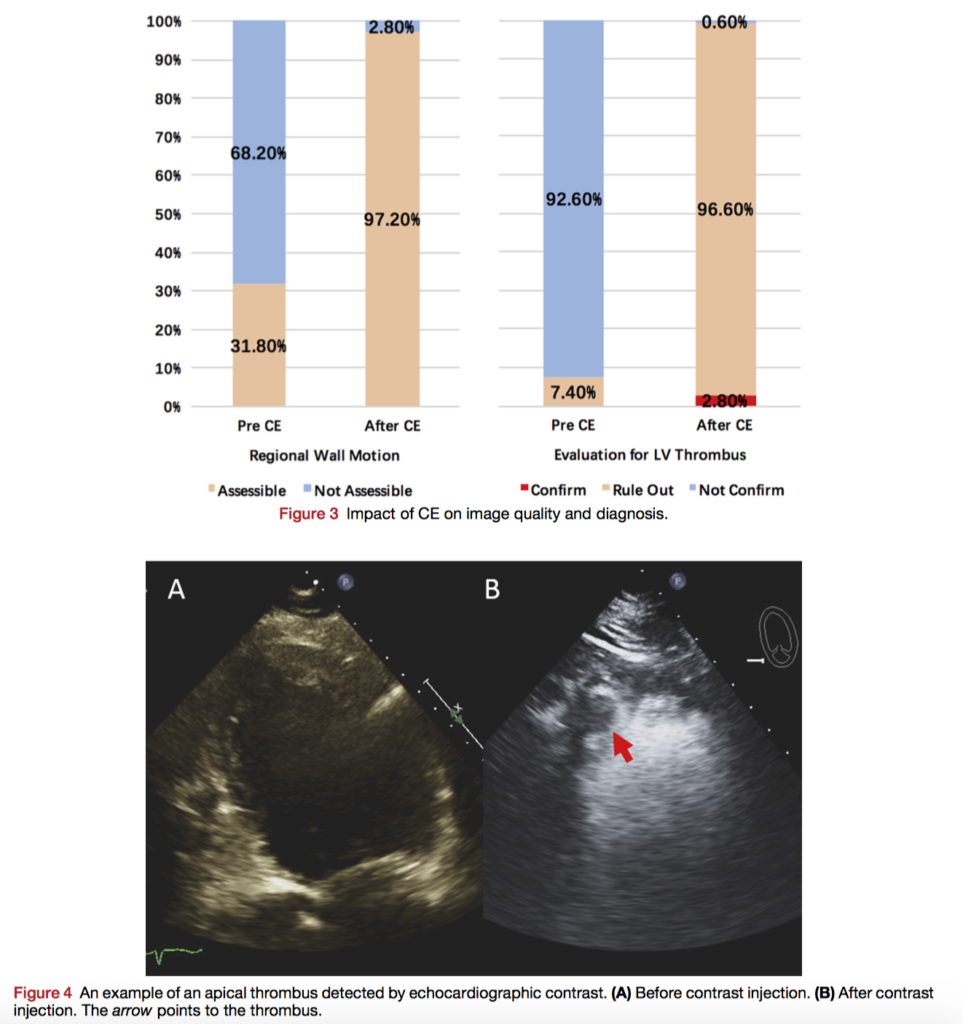
Use of contrast-enhanced echocardiography (CE) remains low, despite current recommendations and evidence it may alter clinical decision making in inpatients. Given the low uptake, are there specific populations which may benefit from targeted increased use? In this prospective trial, 176 patients with technically difficult transthoracic echocardiography who received CE per current recommendations were enrolled. Changes in overall management occurred in 51% of patients, with no significant difference between inpatients and outpatients (60.0% vs 48.1%, respectively, P = .225). However, patients with heart failure, cardiomyopathy, and arrhythmia did have a higher proportion of changes in management. In addition, a left ventricular ejection fraction (LVEF) of <50% before CE was a significant predictor of change of management after CE (p=0.004). The authors suggest CE does alter management, especially in those with low LVEF.
Perioperative Medicine
Summarised by Andrew Haymet
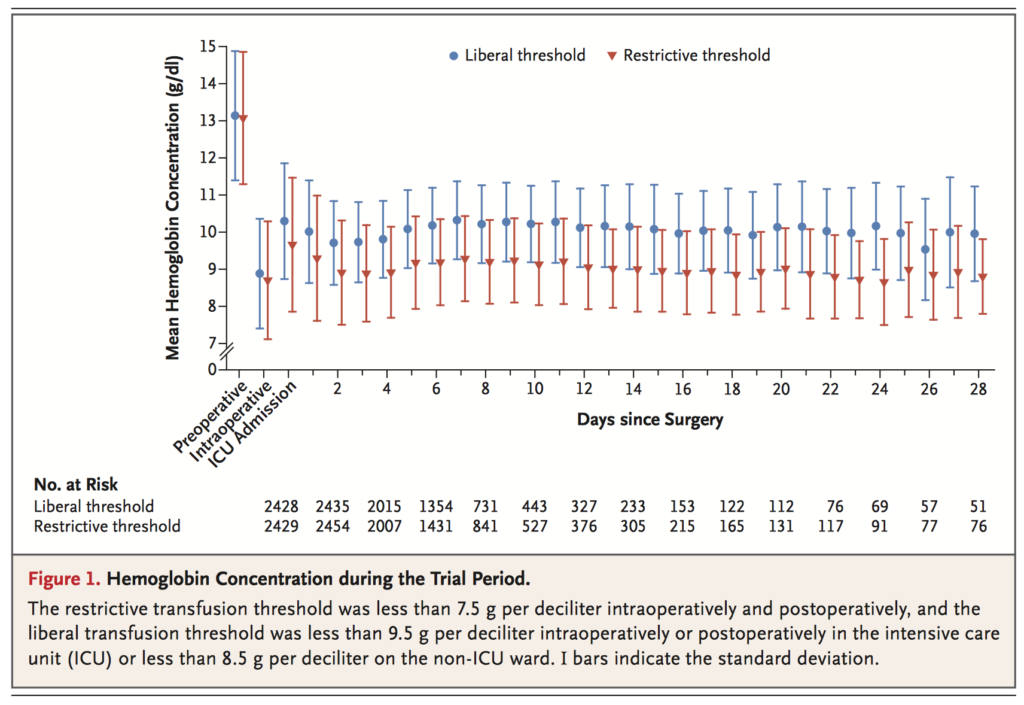
The effect of restrictive versus liberal red-cell transfusion strategy on clinical outcomes in patient outcomes remains unclear. This multicenter, open-label, noninferiority trial randomly assigned 5243 adults undergoing cardiac surgery who had a EuroSCORE of 6 or more to a restrictive (transfuse if haemoglobin <75g/L starting from induction) or a liberal red-cell transfusion threshold (transfuse if haemoglobin <95g/L in OR or ICU, or if <85 in a non-ICU ward). Primary outcomes were death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis by hospital discharge or day 28, whichever was first. The primary outcome occurred in 11.4% of the patients in the restrictive-threshold group, as compared with 12.5% of those in the liberal-threshold group (absolute risk difference, −1.11 percentage points; 95% confidence interval [CI], −2.93 to 0.72; odds ratio, 0.90; 95% CI, 0.76 to 1.07; P<0.001 for noninferiority). The authors concluded that a restrictive strategy regarding red cell transfusion was noninferior to a liberal strategy with respect to the composite outcome of all-cause mortality, MI, stroke, or new onset renal failure with dialysis, with less blood transfused.
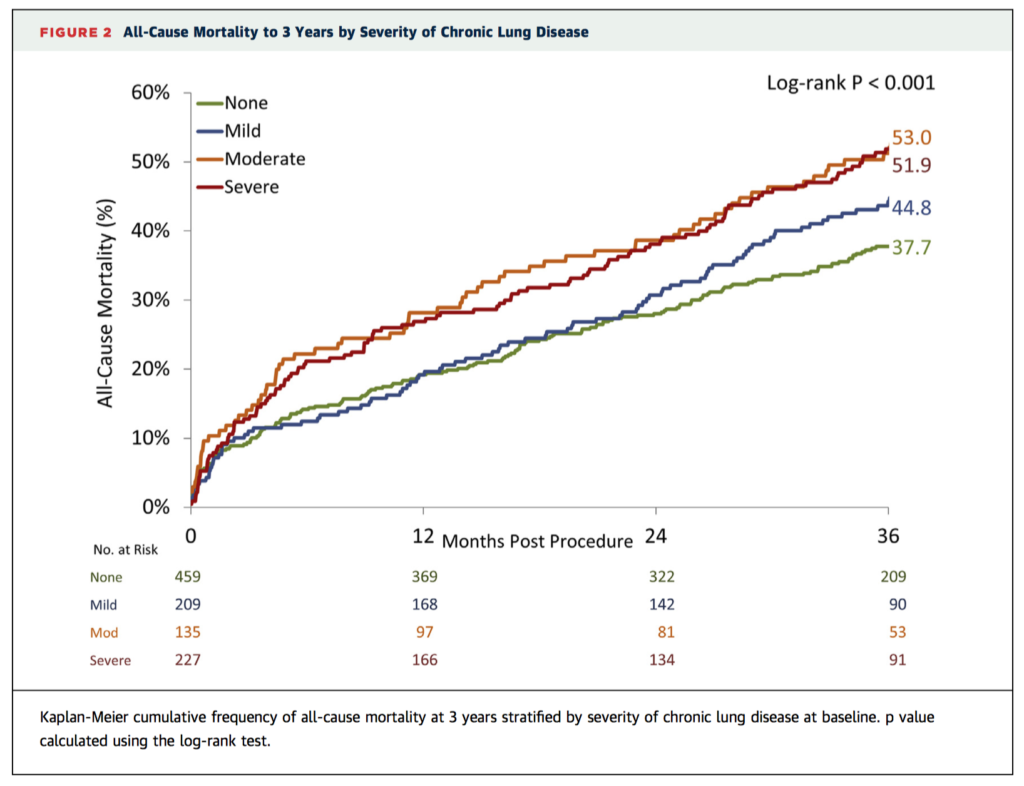
The long term effect of chronic lung disease (CLD) after transcatheter aortic valve replacement (TAVR) is unknown. This study of 1,030 patients aimed to characterize the long term effect of CLD on mortality, clinical outcomes, quality of life, and health benefits after TAVR with a self-expanding bioprosthesis. Clinical outcome and health status were assessed using the Kansas City Cardiomyopathy Questionnaire overall summary score (KCCQ-OS). CLD was present in 55% (20% mild, 13% moderate, 22% severe) of the 1,030 patients studied. All-cause mortality was higher in patients with moderate and severe CLD at 1 year (19.6% mild, 28.1% moderate, 26.9% severe CLD vs. 19.2% non-CLD; p ¼ 0.030) and 3 years (44.8% mild, 53.0% moderate, 51.9% severe vs. 37.7% non-CLD; p < 0.001). The authors concluded that moderate and severe CLD increased 1 and 3 year mortality after TAVR. Although functional status and quality of life were improved in CLD at 1 and 3 years after TAVR, a favourable health benefit was only achieved in selected patients.
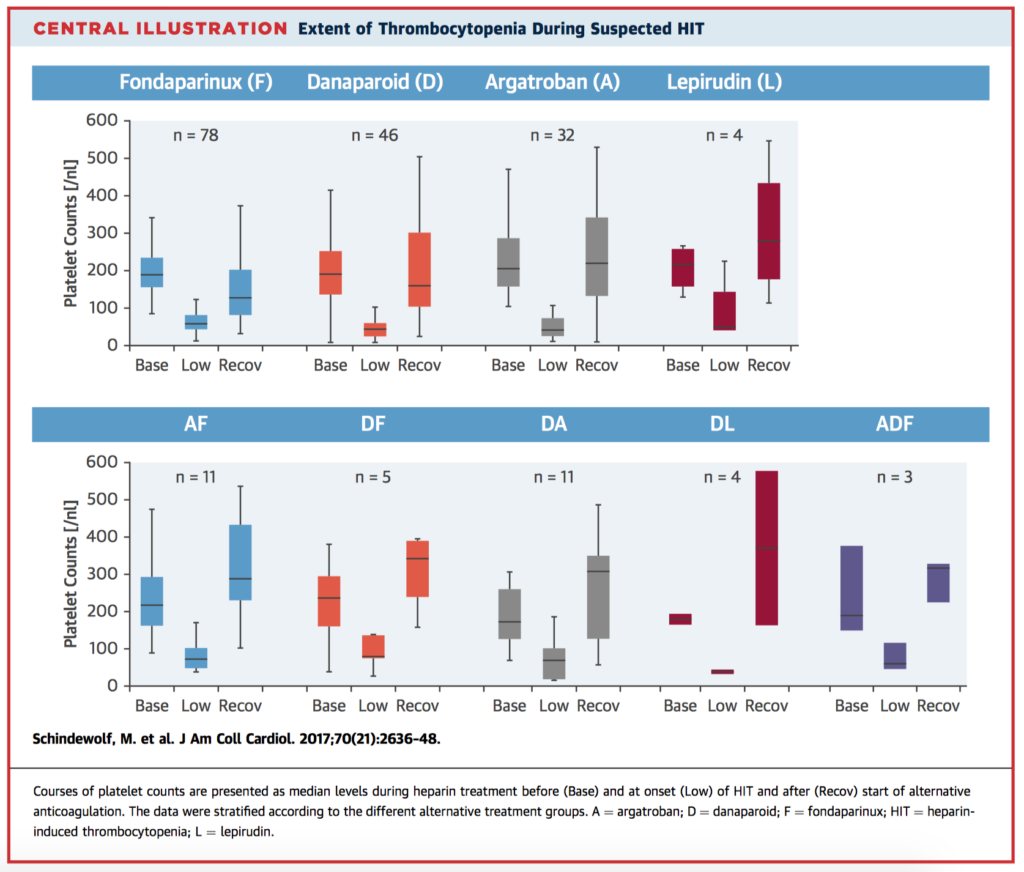
Life threatening heparin-induced thrombocytopenia (HIT) is treated with the alternative nonheparin anticoagulants argatroban, lepirudin, or danaparoid. Frequently, fondaparinux is used off label. This national, multicentre registry study aimed to establish the safety and efficacy of the different anticoagulants for treating HIT in 195 hospitalized patients diagnosed with HIT. Main outcome measures were incidences of HIT-specific complications (thromboembolic venous/arterial events, amputations, recurrent/persistent thrombocytopenia, skin lesions), and bleeding. The composite endpoint of HIT-specific complications (thromboembolic events, amputation, skin necrosis) occurred in 11.7% of patients treated with approved alternative anticoagulation and in 0.0% of fondaparinux-treated patients. The all-cause in-hospital mortality rates were 14.4% during approved alternative anticoagulation and 0.0% during fondaparinux treatment. Bleeding complications occurred in alternatively anticoagulated patients and in fondaparinux-treated patients in 6.3% and 4.8%, respectively. Fondaparinux was found to effective and safe in suspected acute HIT; no HIT-specific complications occurred in patients treated with fondparinux, even among those with a high clinical HIT probability.